 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
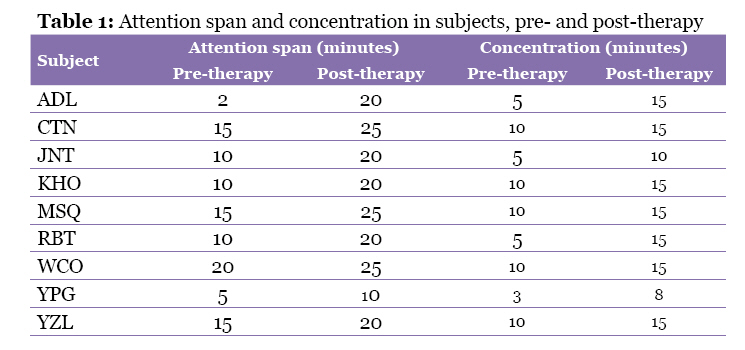
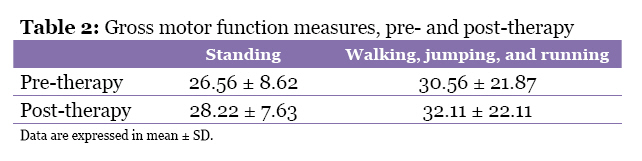
Malaysian Journal of Medical Sciences, Vol. 17, No. 3, 2010, pp. 1-4 Editorial The Confluence between Arts and Medical Sciences: Music and Movement Therapy for Children with Cerebral Palsy Mohamed Ghouse Nasuruddin School of Arts, Universiti Sains Malaysia, 18000, Pulau Pinang, Malaysia Correspondence: Professor Emeritus Dato’ Mohamed Ghouse Nasuruddin, BA, Dip Ed, MA, PhD (Indiana), School of Arts Universiti Sains Malaysia, 18000 USM, Pulau Pinang, Malaysia, Tel: +6013-420 6000 Fax: +604-656 0461 Email: mdghouse_nasuruddin@yahoo.com Code Number: mj10025 The arts, specifically music and movement, are normally identified as serving an aesthetic function, principally that of entertainment. Their function as a therapeutic tool, however, is often neglected or, at the very best, misunderstood. The arts have been used by traditional societies in healing ceremonies to address psychosomatic maladies. These societies believed that all ailments were attributable to spiritual misalignment; therefore, there was a perceived need to placate the spirits through the use of music and movement in order to redress physiological and psychosomatic conditions. Such therapeutic healing was common in early societies and is still common even in advanced societies, such as Malaysia; it is still being practised in Kelantan and Terengganu, in the form of “Main Puteri” and “Main Bageh”. In modern society, the arts have been known to relieve stress and promote a sense of well-being as well as to improve a person’s physical and mental faculties (1). The act of indulging in artistic activities, such as music, dance, drama, or painting, that are both verbal and non-verbal forms of expression allows the body and mind to activate internal energy in creating an aesthetic expression. This manifestation of the inner self has a cathartic, cleansing, and calming effect: relieving stress, muscular strains, and cerebral tension. Similarly, such therapeutic effects can be elicited through artistic involvement in special children who suffer from motor and/or cognitive deficiencies (2–5). In such cases, the goal is to activate and deploy this internal energy to extend the range of their motor functions and improve their cognitive faculties as well as to foster a sense of achievement and self-fulfilment. To explore the efficacy and viability of therapy that brings the confluence of the arts and sciences into focus, a pilot study was instituted by Ms Maria Soccoro of the Department of Neuroscience, School of Medical Sciences, Universiti Sains Malaysia, and myself. The study focused on the use of gamelan (a form of traditional music) to gauge and improve the gross motor functions of children with cerebral palsy (CP). For this project, we solicited the cooperation of The Spastic Centre in Penang, a day school for children with varying severities of CP (those diagnosed with diplegic, hemiplegic, monoplegic, athetoid, and ataxic CP). It was originally proposed to have 2 groups of 15 children each for a total of 30, the objective being to have 1 control and 1 intervention group. However, the centre did not have enough children of mild spasticity with acceptable cognitive level (i.e., able to follow and understand instructions) to fill these 2 groups. Nevertheless, Ms Soccoro, a neuro-psychologist, conducted a preliminary assessment of the sample patients using the Wechsler Abbreviated Scale of Intelligence (performance scale) test and the test for reception and grammar. Dr Abdul Rahman Ghani, a neurosurgeon, conducted the Gross Motor Function Measure (GMFM-66) analysis to select appropriate study subjects. The GMFM-66 test quantitatively evaluates 5 dimensions: lying and rolling; sitting; crawling and kneeling; standing; and walking, running, and jumping (6). Based on these tests, 9 patients with parental informed consent were selected: 5 diplagic, 1 tripelagic, and 3 others with full ambulatory function and both arms functional. The patients were all mobile but not stable. Their age ranged between 7 and 12 years, with a receptive language level of 4.00 to 4.11 years. It was agreed that the therapy would be administered 2 days per week (Monday and Friday) for the duration of the project. Each session lasted for 1 hour from 9:00 to 10:00 am; this time coincided with the children’s exercise period. For these sessions, The Spastic Centre transported the students to and from the Gamelan Studio, School of Arts, Universiti Sains Malaysia, where the therapy was administered. The therapeutic intervention was designed around the use of music, movement, and theatre games. Gamelan music was used as part of the intervention. Almost all of the patients had not seen or experienced the hearing or playing of gamelan. This type of musical ensemble consists of large- and medium-sized circular knobbed gongs and bronze plates of varying pitches, all arranged in pentatonic scale sequence and suspended over a trough-like resonator (7). These musical instruments can be easily handled and do not require any fine technical skill, as do playing the violin, piano, or flute. The basic skill required is the ability to strike the instruments on the knob of the gong or at the centre of the metal plates. These are all percussive instruments. We were not concerned about the colour, timbre, or tonal quality of the sounds produced. Our focus was the striking actions that anyone can execute, even the special children with various degrees of spasticity. The initial objective was to get them to produce sound and by doing so getting them to exercise their arms and hands, with the purpose of relaxing and extending the range of their muscles. Warm-up sessions included basic hand motions (raising upwards, sideways, lowering the arms from the top position to the floor, slapping the floor, vibrating the fingers, swinging from side to side, and clapping) and leg movements (simple straightening exercise in a sitting position and then retracting them, wiggling the toes, bending the knees, flexion, and pronation). Head movements were introduced, together with 4-point and 2-point crawling movements, as well as rolling from side to side. We also included vocal inflexion, shouting, and making specific animal sounds. Theatre games, such as imitating various animal movements, story-telling and magic shows, were also incorporated. For the first few sessions, we worked towards obtaining their trust and confidence and creating a relaxed and friendly atmosphere; we did not have any specific targets at this time, intending rather to improvise as we go along to meet their interests. We worked within the general framework of playing the musical instruments and executing movements, however, and we observed the following improvements in the children after the intervention: 1. Improvement in Posture Subject ADL voluntarily corrected his posture without being reminded and then sat with good posture. Similarly, subject CTN self-corrected her posture and could tolerate cross-legged sitting for almost an hour, whereas previously she could only sustain it for 15 minutes. Subject JNT improved her cross-legged sitting from 5 to 10 minutes. Subject YPG had such difficulty in sitting upright that when he first arrived, he had to be supported. After undergoing therapy, however, he sat unsupported without fear and was able to maintain upright posture for 15 minutes. Subject WCO was also able to maintain upright posture. Subject KHO normally would not tolerate sitting on the floor, but he was able to sit on the floor for almost 10 minutes. The sitting position of subject YZL had improved, and she had been able to maintain it for almost 20 to 30 minutes. 2. Improvement in Attention Span and Concentration Almost all of the children have shown improvement in attention span and concentration (Table 1), ranging from 5 to 15 minutes and 5 to 10 minutes, respectively. 3. Improvements in Gross Motor Function Subject ADL’s active range of motion, grasp, and release on the right side has improved. Subjects JNT and CTN can move their legs into a sitting position more easily and sustain them for a longer period of time. Subject WCO has shown improvement in the quality of movement in her upper limbs and has performed given tasks faster than before. Subject YZL improved the movement pattern of her upper limbs and her fine motor functions. 4. Confidence Level All subjects have shown increased confidence and have been able to execute tasks more effectively. They have each shown a keen interest in attending the therapy sessions. 5. Cognitive Function All subjects have shown memory improvement. 6. Gross Motor Function At post-test, all subjects scored significantly higher on gross motor function as measured by standing (Table 2). They also showed significant improvement over time on the measures of walking, jumping, and running. Mr Santosh, the therapist at The Spastic Centre, Penang, gave an outstanding testimonial on the outcome of the pilot project. The children started the twice weekly (Mondays and Fridays) music and movement therapy sessions in March 2008. They were enthusiastic and keen in attending these sessions. During these sessions, they were instructed to play the traditional gamelan instruments and drums. While playing these instruments, they had to maintain an upright posture and forgot that they were sitting without any support. They showed keen interest in playing these instruments. In playing these musical instruments, the instructor demonstrated the method of striking the instruments, and the children copied them and followed the instructions well. During the movement sessions, which involve various types of normal movements as well as animal movements, the children imitated these movements to the best of their ability. When they were asked to do the same thing at home or in school, they would not be that co-operative. Their co-operative attitude is because they are involved in group tasks and has generated a sense of competition among them. They get so involved and enjoyed doing their tasks that they forgot their physical limitation. For example, when the instructor asked them to move towards him, they do so with their various mode of ambulation, without regard to their physical disabilities. The children attending these sessions have shown improvement in their posture and movement pattern. Even though these improvements are so small, it improves their quality of life in executing the usual daily movements. They have also become more active and self-confident. They also relate their experience in these therapy sessions to their friends who are not attending these sessions. These music and movement therapy has enhanced the children socialising and communication skills. The use of music (gamelan) and movement as a non-invasive therapy in gauging and improving the gross motor functions of children with CP has shown positive results based on clinical and empirical findings. In fact, this therapy has a broader application than solely improvement in the gross motor functions. Besides improvement in posture, muscle strength in the upper and lower limbs, range of motion and the ability to maintain a long period of sitting cross-legged, the subjects have shown improvement in attention span, concentration and confidence. They have also improved their hand-eye coordination and their memory. It is important to mention here that this therapy in no way replaces the subject’s normal medication. The therapy does, however, aid in improving their quality of life and, through the use of music and movement, activates the dormant primordial energy of self-healing within the given configuration of their disabilities. Acknowledgements I would like to thank Professor Dr Jafri Malin Abdullah, the Editor-in-chief, for the opportunity to share my experience in music and movement therapy. My deepest gratitude goes to Ms Maria Soccoro and Dr Abdul Rahman Ghani from the Neuroscience Department, USM, Dr Mumtaz Becker from the School of Arts, USM, Ms Valiammal Allagapan, the administrator of The Spastic Centre, and Mr Santosh, the therapist at The Spastic Centre, for their contributions towards this project. References
© Copyright 2010 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj10025t2.jpg] [mj10025t1.jpg] |
| |||||||||

{kind=link}
{kind=link}