 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
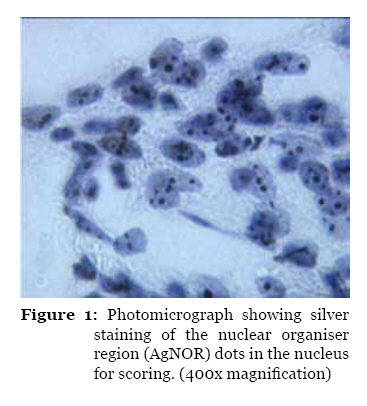
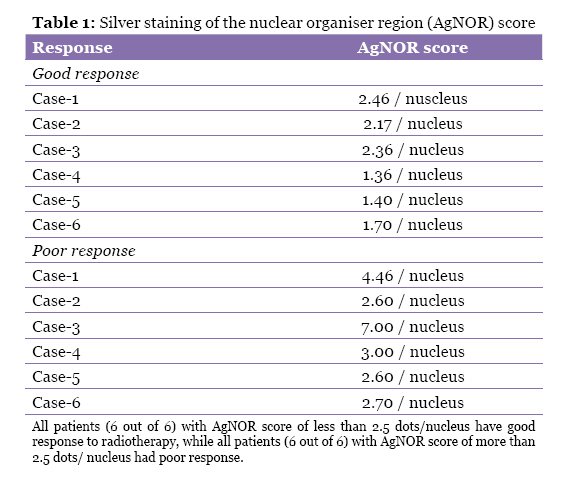
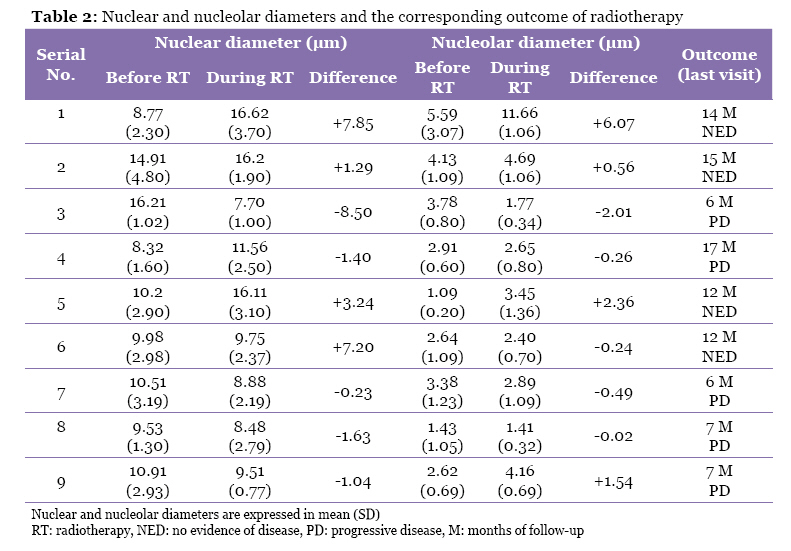
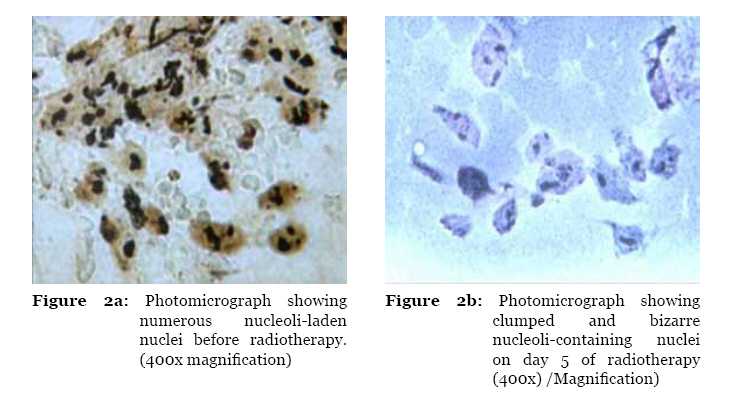
Malaysian Journal of Medical Sciences, Vol. 17, No. 3, 2010, pp. 19-26 Original Article Correlation of Nuclear Morphometry and AgNOR Score with Radiation Response in Squamous Cell Cancers of the Head and Neck: A Preliminary Study Biswa Mohan Biswal1 , Nor Hayati Othman2 1Department of Nuclear Medicine, Radiotherapy, and Oncology, Universiti Sains Malaysia Health Campus, 16150 Kubang Kerian, Kelantan, Malaysia Correspondence: Associate Professor Dr Biswa Mohan Biswal, MBBS, MD, DNB, Department of Nuclear Medicine, Radiotherapy, and Oncology, School of Medical Sciences, Universiti Sains Malaysia Health Campus, 16150 Kubang Kerian, Kelantan, Malaysia, Tel: +609-7676666 Fax: +609-7644416 Email: biswa@kb.usm.my Submitted: 8 Sep 2009 Code Number: mj10028 Abstract Background: Prediction of radiation response before the completion of the radiotherapy schedule is challenging. Information about radiation response could help oncologist to choose the appropriate combination and sequence of therapies in the multidisciplinary management of cancer. Keywords: AgNORs, fine-needle aspiration, squamous cell cancer, radio-sensitivity, radiotherapy, radiology, medical sciences IntroductionHead and neck cancers account for 5%–10% of all cancers (1), and the malignancies have diverse biological behaviours and predictions for treatment response. Surgery, radiotherapy, and occasionally chemotherapy are the core modalities for management of head and neck cancers. Radiotherapy is used in more than 60% of head and neck cancers with the purpose being radical, adjuvant, or palliative care. Not all patients who receive radiotherapy achieve a desirable radiation response. Radio-sensitivity is not uniform, even in the similar histological subgroups in head and neck cancers (2). The response can vary, even when stage, site, tumour volume, and histology are kept constant. Additionally, histopathological subcategories do not show a consistent prediction of radiation response (3). The in vivo cytological test and the cell surviving fraction for a 2 Gy dose of radiation (SF2) are 2 known methods for predicting radiation response (4). Alternate prediction methods use radiation-induced histomorphological changes, especially changes seen in the nucleus, as a marker of radio-sensitivity. However, these methods of predicting radiation response are not practical in clinical oncology due to complicated nature of the tests. In 1947, Graham introduced the concept of predicting radio-sensitivity using the radiation response test (5). Previously, serial cytology slides were studied to assess the radio-sensitivity of various cancers; following radiotherapy, multinucleation, and nuclear enlargement of the malignant cells were common observed changes. Past radiobiological studies have shown that induction of cell multinucleation is dose-dependent and correlated with cell survival assay, which suggests that they are non-clonogenic (6). Radiation can induce the fragmentation of the chromosome or the formation of abnormal chromosomes, which do not take part in mitosis. These chromosomal fragments are called micronuclei, and their induction is dose-related and correlated with survival of cancer patients (7,8). Under high magnification, it is possible to observe the nuclear and nucleolar morphometry using a computer-assisted image analyser (9). These nucleolar events can also be demonstrated with silver staining of the nuclear organiser region (AgNOR). Nuclear organiser regions (NOR) are loops of ribosomal DNA located in the short arm of chromosomes 13, 14, 15, 21, and 22, and transcribe to ribosomal RNA. NOR vary in size and shape according to the nucleolar transcription. Interestingly, they are related to the cell cycle and may also be related to cell proliferation. Binding of silver and protein occur in carboxyl and sulfhydryl groups by colloidal precipitating ionic silver. The carboxyl group on the protein reduces the silver solution that forms the micronuclei of silver. The large aggregate of silver is deposited on the disulfide and sulfhydryl group sites; they are easily observed using light microscopy. An increase in the AgNOR score suggests an increase in ribosomal activity. Studies of the predictive index based on AgNOR score are effective as early as after the first fraction of radiotherapy; the AgNOR score is correlated with local control of the disease by a full radiotherapy protocol. Knowledge of the probability of radiation response before the completion of radiotherapy would allow re-evaluation of therapeutic options (10). The nuclear roundness factor (NRF), detectable by an image analyzer, is another parameter that has been demonstrated to predict radiation response in Wilms’ tumour and prostate cancer (11,12). In this study, we examined the AgNOR score as well as nuclear and nucleolar morphometry before and during radiotherapy as a predictor of radio-sensitivity. Materials and Methods Patient selection A total of 26 patients with documented cases of squamous cell cancers involving the head and neck region were recruited for this study. The general physical examination, clinical tumour volume, biochemical investigation, and radiological evaluation were recorded on a case report form for analysis. The clinical tumour volume was measured as the maximum diameter in centimetres in 3 dimensions. The tumour volume was measured before (day 0), during (on 5th fraction), and after radiotherapy (on 10th fraction), as well as 6 weeks after initiation of radiotherapy. Radiotherapy scheduleRadiotherapy was delivered with a 6 MV linear accelerator, using a 2- or 3-field technique. The radiotherapy schedule consists of 30 Gy in 10 fractions over a 2-week period: treating 5-day-a-week with 2-day break during the weekends. For cases of parallel-opposed portal, the dose was calculated at the mid-plane, but in the lower neck field, dose was calculated at the maximum depth dose (d-max). Individualised thermoplastic moulds were prepared for daily reproducibility of set-up for upper neck region tumours. The radiation dose was kept uniform in all cases, and we expected a similar outcome with this schedule. Patients with good radiation response were subjected to further radiotherapy doses (30 Gy in 10 fractions over a 2-week period) as part of a split-course technique following the exclusion of sensitive structures. At the end of radiotherapy, the response to radiotherapy was evaluated as complete response (CR), partial response (PR), or progressive disease (PD). The AgNOR scoring and nuclear morphometry was performed regardless of an additional Phase II radiotherapy course, and the last cytology sample was collected on the 6th week, counted from day 1 of the radiotherapy course. Cytological evaluationFine-needle aspiration cytology (FNAC) was performed to obtain tissue materials. The tissue fluids were obtained from the measurable nodes, which were in the radiotherapy portal. The FNAC was performed before starting radiotherapy (day 1), at day 5 (after 5th fraction) of the treatment, at end of radiotherapy (after 10th fraction) and 6 weeks post-radiotherapy, counted from day 1 of radiotherapy. The AgNOR staining was performed according to the modified Crocker method (13). The cytology samples were smeared on conventional glass slides with frosted ends and then immersed in 95% alcohol as the fixative. The slides were rinsed with xylene 3 times for 5–10 minutes and then treated with 100% ethanol for 2–5 minutes. Next, the slides were washed with tap water for 5 minutes and rinsed with deionised water 2–3 times for 3 minutes. The slides were incubated in the dark for 60 minutes with 1 volume of solution-A and 2 volumes of solution-B, and then rinsed with deionised water. Solution-A (colloid developing solution) consisted of 100 ml pure water, 2 g gelatine, and 1 ml formic acid. The gelatin was dissolved by stirring at 40–60 °C for 10–20 minutes. The solution was left at a room temperature of 40 °C. Solution-B contained 100 ml pure water and 50 g silver nitrate and was protected from light by wrapping aluminium foil around the container. The slides were washed with 5% sodium thiosulfate solution for 5 minutes followed by rinsing with 100% ethanol and, subsequently, xylene. The stained slides were then mounted with a cover slip. The AgNOR stained as black dots within the nucleus. The number of AgNOR dots were counted in 100 cells, and the mean AgNOR count (AgNOR score) was calculated for each case. Each cytology slides were subjected to nuclear morphometric analysis using a computer assisted image analyser (Leica Qwin, Germany) at 400x magnification. The nucleus and nucleolus diameters were determined by this method. Statistical analysisThe data obtained from the study were evaluated using SPSS version 11 (SPSS Inc, Chicago, IL). The demographic data were tabulated, and the median value of the AgNOR score, nuclear diameter, and nucleolar diameter were measured. The outcomes, in terms of radiation response, were analysed against the baseline AgNOR score and nuclear morphometry data. The difference in nuclear and nucleolar diameters on day 1 and day 5 were compared to the radiation response using the Mann–Whitney test. ResultsAs per the protocol, the 26 patients who completed the radiotherapy schedule consisted of 6 females and 20 males. The median age of the patient population was 44 years. Although we attempted aspiration cytology in all 26 patients, cellular materials were evaluable for only 9 patients for nuclear morphometry and 12 patients for AgNOR score. The failure to determine the nuclear morphometric and AgNOR score in other cases were due to sampling error, failure to obtain cellular material, and quick tumour regression after brief radiotherapy. The primary tumours were distributed in the nasopharynx (n = 11), larynx and hypopharynx (n = 5), metastatic neck nodes (n = 4) and miscellaneous tumours (n = 6) of the head and neck sub-sites. RadiotherapyOut of 26 patients evaluated, 14 patients (54%) achieved CR, 6 patients achieved PR (23%), and the remaining 6 had PD (23%) following radiotherapy. Cytology evaluationSampling was done in 54 attempts; however, only 33 aspirate yield cellular materials. After a few fractions of radiotherapy, patients showed good response to radiation, which made it difficult to obtain good tissue samples on the 2nd and 3rd FNAC procedure. Out of 26 patients, 20 patients (76%) underwent initial cytology (cytology-1), which yielded good cellular material; 10 patients (38%) yielded good cellular aspirate after day 5 of radiotherapy (cytology-2); and only 3 patients (12%) had successful 3rd round cytology. The cytology from 6th week aspirates was not successful in some cases due to sampling error and regression of the tumour following radiotherapy. AgNOR scoreManual AgNOR score was done for 33 slides by counting the number of AgNOR dots per the given number of nuclei counted (Figure 1). Baseline AgNOR scores were available in 12 patients. The baseline mean AgNOR score was 3.0, range 1.2–7.0, and the mean AgNOR score on day 5 of radiotherapy was 2.4, range 1.2–7.1. Patients with a high baseline AgNOR score showed higher treatment failures than those with low baseline AgNOR scores. All patients, 6 out of 6, with AgNOR scores of less than 2.5 achieved a good response to radiotherapy compared with 6 out of 6 patients with AgNOR scores of more than 2.5, who achieved a poor response to radiotherapy (Table 1). Nuclear and nucleolar morphometry The largest nucleus and nucleolus diameters were measured. The average nucleolus diameter was 2.92 μm, range 1.09–11.66 μm, and nucleus diameter was 11.073 μm, range 7.70–16.6 μm. When the nuclear diameter increased from the baseline diameter on day 5 of radiotherapy, there was improved radiation response, local control, and longer survival (Table 2). Following radiotherapy the morphology of the nucleoli in nucleus on day 5 becomes more clumped and bizarre compared to baseline features on day 1 as shown in Figure 2. There was no correlation between nuclear/nucleolar diameters with 3-dimensional clinical tumour volume of the target lesion. When comparing the changes in nuclear diameter on day 5 to the baseline diameter, there was statistically significant improvement in radiation response that correlated with a positive increase in diameter (P = 0.016). A similar comparison was done with nucleolar changes; however, the result did not yield any correlation (P = 0.111). Follow-upThe patients were advised to attend a regular follow-up at 2-month intervals for the first 2 years and then at 3-month intervals thereafter. The follow-up consisted of a clinical examination; however, radiological evaluation was performed at every 6-month interval. The median follow-up interval was 7 months, range 4–20 months. DiscussionThis is a prospective study to evaluate the value of AgNOR score as well as nuclear morphometry before and during a course of fractionated radiotherapy to predict radiation response. This study, even though it had a small sample size, showed that an increased trend in the nuclear diameter on day 5 compared to baseline was associated with a favourable response to radiotherapy. Furthermore, an increase in baseline AgNOR score of more than 2.5 was associated with radiation failures at a median follow-up duration of 7 months, range 4–20 months. AgNOR count per nucleus is being used in many cancers to predict response to radiation therapy and/or outcome of treatment. In a 10-patient study, Kossard et al AgNOR dots per nucleus in small cell melanoma. They found a variation of AgNOR count: 5.83 in small cell melanoma, 8.49 in superficial spreading melanoma, and 2.71 among dermal nevi (14). This suggests that a higher AgNOR score predicts an aggressive tumour. A similar pattern was observed in our study; those cancers with a high AgNOR score per nucleus showed high failure rates. A similar study, performed by Yue et al., also showed hyperactivity of malignant cells in head and neck cancers with a high AgNOR score (15). In contrast, a study from Japan demonstrated that a higher AgNOR score correlated with a good radiation response to pre-operative radiotherapy for oral cavity cancers (16). The nucleus and nucleolus are the main targets for radiation injury, whether the tumour is malignant or benign. Under a light microscope, the nucleolus appears as a dot-like structure positioned at the centre of the nucleus or slightly displaced towards the inner side of the nuclear membrane. A nucleolus is present in either a reticular array or as compact structures, and it has a fibrillar centre, a vacuolar portion, and a nucleolus-associated chromatin. Thus, a nucleolus consists of dense fibrils and granules, which appear as a dark staining area of varying intensity (17). A nucleolus is responsible for ribosome production and transcription of rRNA and is very sensitive to a change in ribosomal DNA synthesis. Cytochemical studies have shown a marked increase in the amount of AgNOR scores with large nucleoli that implies a higher level of ribosomal production. In our study, the nucleolus mean diameter was 2.92 mm, range 1.09–11.66 mm. However, there was no statistical correlation with treatment outcome. Radiation therapy treatment is based on tumour factors such as location, size, and histological grade. Patients with stage III and IV head and neck cancers are treated with a fixed dose of radiation, but an increasing body of evidence shows that the response to radiation is not constant, even if the tumour-related variables are held constant. This wide variation of the radio-responsiveness to fractionated radiotherapy is probably indicated by an inherent cytological factor influencing the behaviour of the cancer after radiation exposure. Fibroblasts from patients suffering from ataxia telangiectasia are 2–3 times more sensitive than the normal cells (2). Thus, the radiation response is a product of a wide range of cellular parameters (e.g., nuclear, nucleolar, chromosomal, and genetic factors, and apoptosis). Cancers are commonly classified according to histology and graded according to the degree of their differentiation: well-differentiated, moderately differentiated, and poorly differentiated. The poorly differentiated cancers seem to be more sensitive to radiation than well-differentiated malignancies. These histology-based variations are demonstrated in cervical cancers and some head and neck cancers. Sometimes, histopathology does not correlate with clinical curability (3). In our study, we did not find any correlation between the histopathology grade and response to radiotherapy. Colony assay of the tumour cells has been proposed for predicting radiation response based on the fraction of cells surviving a particular radiation dose, which is defined as the ability to undergo at least 6 doublings. Intrinsic radio-sensitivity measurements with SF2 analysis have been demonstrated by Fertil and Malaise, who analysed the published studies of in vitro radio-sensitivity of tumour cell lines from different histological types and found a general correlation with clinical curability (18). West et al. studied the SF2 assay of radiotherapy-treated squamous cells of cervical cancers. In vitro tumour SF2 values from fresh biopsy material using colony formation in agar were correlated with the treatment outcome. Patients with an SF2 value higher than the median value, 0.40, had a significantly lower survival rate than those with an SF2 value below the median (4). An ideal radiation sensitivity test should be specific, sensitive, cost effective, and able to be practiced routinely. The chromosomal damage assay and radio-sensitive gene assay are two new tools for the prediction of radio-sensitivity (19). The first study of a radio-sensitivity test was demonstrated using the serial cytology tests from cervical cancer, called Grahms grading (5). Subsequently, the studies have been duplicated by Gupta et al. (20). Following a course of radiation, there is alteration in the cellular and nuclear morphology. There may be an increase in nucleus size, whereby the nuclear material becomes more condensed with the appearance of prominent nuclei. Bhattathiri et al. studied serial cytological features for the analysis of micronuclei formation during fractionated radiation on squamous cell cancers of the oral cavity. They found a positive correlation between micronuclei formation and treatment outcome (21). Nuclear morphometric analysis is a quantitation method that has been successfully employed in predicting treatment outcomes for a number of malignancies. Nuclear and nucleolar size estimation is a new concept for the assessment of tumour radio-sensitivity. McLean et al. (9) were some of the early researchers in this area; they found a correlation between large nucleoli and patient treatment outcome. In the study on induction of micronucleation, nuclear budding, and multinucleation produced by fractionated radiotherapy, Bhattathiri et al. showed that multinucleation had the greatest relation with radiation sensitivity. This study suggested that the injury to the cytokinetic apparatus was important in determining tumour radio-sensitivity (21). Another study by Memon et al. also demonstrated nuclear changes as a predictor of radio-responsiveness in oral cancer patients following radiotherapy (22). In our study, we measured the diameters of the tumour cell nuclei before and during a fractionated course of radiotherapy. Those patients who showed an increase in the nucleus diameter following radiotherapy achieved good local control of disease compared with those who showed a decreased size. Following an initial course of radiotherapy, the nucleus of the cell increases and gradually becomes fragmented, which causes reproductive cell death. Another dimension of radio-responsiveness is the nuclear roundness factor (NRF). In a study on prostate cancers, Hurwitz et al. noticed a positive correlation of NRF with radio-sensitivity (12). The authors used an automated imaging device to determine NRF. Sampling from aspiration cytology is an optimal method to evaluate nuclear morphometric features (23), but studies using conventional haematoxylin–eosin histology slides to determine nuclear morphometry have also been successful (24). In our experience, the failure to obtain cellular samples during radiotherapy is high, and it is more marked during subsequent aspiration cytology when the tumour is regressing. Conclusion The inherent radio-sensitivity to the tumour cells, the proportion of the hypoxic cell component and repopulation by the resistant clones of cells govern cancer response to radiation. The first component of radio-sensitivity can be predicted using nuclear morphometry before and during a course of radiotherapy. In borderline clinical situations, where the decision to use either radiotherapy or surgery is uncertain, nuclear morphometry test might help to decide the treatment arm before completion of radiotherapy. However, a study on a large number of patients needs to be done before it can be recommended for clinical practice. Acknowledgements This work was supported by the short-term grant of Universiti Sains Malaysia (grant number 1039/9036/1039). The authors appreciate the contributions rendered by Mr Nik Ruzman Nik Idris (medical physicist), Mr Rozaimey (radiotherapist), and Ms Mariam Azmi (cytopathology technologist) to carry out this study. Authors’ Contributions Conception and design, final approval of the article: BMB Collection and assembly of data, analysis and interpretation of data, drafting of the article, critical revision of the article: BMB, NHO References
© Copyright 2010 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj10028t1.jpg] [mj10028f2.jpg] [mj10028f1.jpg] [mj10028t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}