 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 17, No. 3, 2010, pp. 48-54 Original Article The Risk Factors of External Ventricular Drainage-Related Infection at Hospital Kuala Lumpur: An Observational Study Mohamad Azhari Omar1, Mohd Saffari Mohd Haspani2 1Department of Neurosciences, School of Medical Sciences, Universiti Sains Malaysia Health Campus, 16150 Kubang Kerian, Kelantan, Malaysia Correspondence: Dr Mohamad Azhari Omar, MD (UKM), MSurg Neurosurgery(USM), Department of Neurosciences, School of Medical Sciences, Universiti Sains Malaysia Health Campus, 16150 Kubang Kerian, Kelantan, Malaysia, Phone: +609-766 4240 Fax: +609-764 8613 Email: azharineuro@yahoo.com Submitted: 4 Aug 2009 Code Number: mj10032 Abstract Background: External ventricular drainage (EVD) has been widely used for the purpose of cerebrospinal fluid (CSF) diversion at Hospital Kuala Lumpur (HKL). Keywords: cerebrospinal fluid shunts, hydrocephalus, in-dwelling catheters, infection, medical sciences Introduction External ventricular drainage (EVD) has become an excellent adjunct to measure the intracranial pressure (ICP) in severe head trauma. The technique also represents an important tool to manage patients with diseases associated with hydrocephalus. However, the main disadvantage of EVD is the risk of contracting a ventriculostomy-related infection (VRI), which has been reported to affect 0.0%–21.9% of patients (1–11). One of the major indications for EVD insertion is hydrocephalus secondary to intraventricular or subarachnoid haemorrhage. Previous studies have shown that patients with blood in the CSF system have a higher rate of EVD infection compared with those with blood-free CSF (4,5,12). Generally, as is common in other surgical practices, factors that are crucial to the risk of infection include the surgeon’s experience, the venue of the procedure, and the surgical technique. The need to remove the initial EVD and reinsert the new catheter after a certain amount of time has elapsed is currently under debate. This is a prospective observational study of the surgical technique in relation to the extra-cranial length of the catheter and other factors among patients subjected to EVD insertion. This study is meant to determine the association of predisposing factors with EVD-related infection over a period of 2 years in the Neurosurgical Department, Hospital Kula Lumpur (HKL). The main purpose of this study was to determine whether the length of the ventricular catheter from the burr hole of the skull to the site of exit will show any significant difference in terms of central nervous system (CNS) infection rate. Other measures, such as the duration for which catheters have been in situ, the surgeon’s experience, the venue at which the procedure was performed, as well as the primary pathology or aetiology that required drainage, were analysed to identify any correlation with infection rate. A total of 87 patients who fulfilled the criteria were included in this study. Statistical analyses (Pearson chi-square test, Fisher’s exact test, and multiple regression test) were performed to determine the associations between EVD-related infections and surgical methods as well as other related factors. Materials and Methods This was an observational prospective study of patients who were admitted to the Neurosurgical Department and underwent the initial EVD insertion at HKL over a period of 2 years (2006–2008). Patients were selected according to the inclusion and exclusion criteria. Inclusion criteria
Exclusion criteria
Data were collected by a single investigator to minimise the risk of error in the evaluation of specific data needed for the study. After patient selection and data collection, the length of tunnelling between the burr hole and the exit skin was measured. The measurement was performed post-operatively using the digital palpation method. The patients were classified as having EVD-related infection if the following criteria were fulfilled (13):
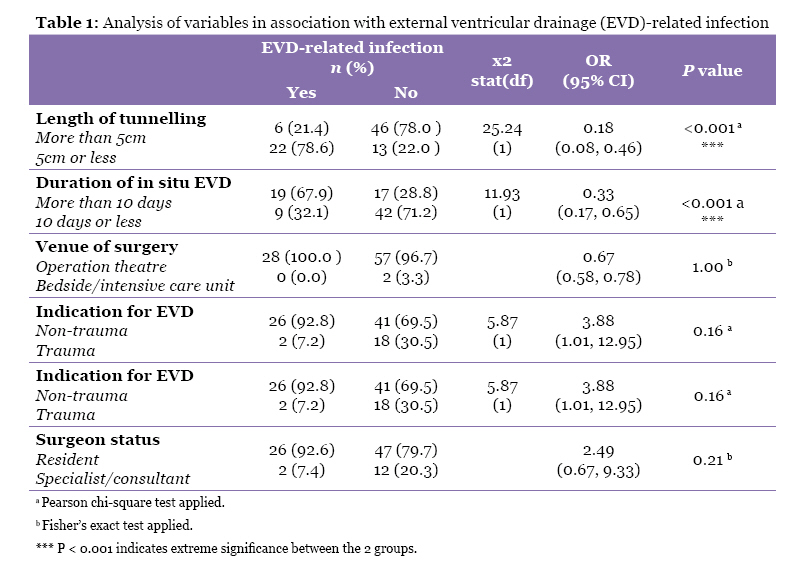
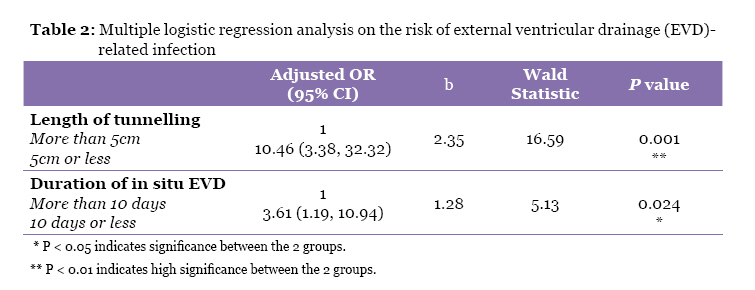
The time of infection was recorded as the time when the sample was obtained. Patients were not classified as having EVD infections if only an isolated CSF culture was positive but other parameters were within normal values. Analyses of the data were done using SPSS version 12.0 (SPSS Inc, Chicago, IL). Descriptive analysis was performed for all variables. The univariate analysis was performed using the chi-square test or Fisher’s exact test, and multiple regression analysis, with P < 0.05 considered to be significant. Results From December 2006 to December 2008, there were more than 400 cases of EVD insertion at HKL. The strict inclusion and exclusion criteria previously outlined yielded a database of 87 patients for analysis. The youngest patient was 14 years old and the oldest was 73 years old. The median age of the patients was 50 years old, with an interquartile range of 27.0. The age group of 50–59 years old comprised the most patients (n = 20). The ventriculostomy insertion procedure was noted to be slightly more common in female patients. Out of 87 cases, 47 patients (54.0%) were female and 40 patients (46.0%) were male. The female to male ratio was 1.17:1. Hypertensive bleeding with intraventricular extension associated with hydrocephalus is the common cause of EVD insertion (28 patients, 32.2%), followed by subarachnoid haemorrhage (25 patients, 28.7%), and ICP monitoring in trauma cases (20 patients, 23.0%). Brain tumour and other factors (including posterior fossa and supratentorial ischaemia or infarct) were the least common indication for EVD insertion. Among the population surveyed, 28 patients (32.2%, 95% CI 23.3% to 42.6%) were diagnosed with EVD-related infection, whereas 59 patients (67.8%) were not infected. The ratio of infected to non-infected patients was 1:2.1. Most patients with EVD-related infections were female. However, for non-EVD-related infections, the numbers of cases were similar among males (31 patients) and females (28 patients). There were less EVD-related infections in the group subjected to tunnelling of more than 5 cm (6 out of 52 patients, 11.5%) compared with the group that required tunnelling of 5 cm or less (22 out of 35 patients, 62.9%). The group of patients subjected to tunnelling of more than 5 cm had a significantly lower risk of EVD-related infection (P < 0.001) compared with the other group, which was subjected to a shorter tunnelling length (Table 1). The bacterial cultures of CSF samples from patients with EVD-related infections showed the presence of various microorganisms: Acinetobacter sp. in 12 patients, methicillin-resistant Staphylococcus aureus (MRSA) in 10 patients, as well as Pseudomanas sp., Enterobacter sp. and Klebsiella sp., which accounted for 3 patients each. In this study, most of the patients who had the EVD in situ for less than 10 days (42 out of 51 patients, 82.3%) showed no evidence of EVD-related infection. EVD-related infection was significantly more common (P < 0.001) among the group subjected to EVD for more than 10 days (19 out of 36 patients, 52.8%). Gram-negative bacteria (12 species) were primarily responsible for EVD-related infections that lasted for more than 10 days. In this investigation, most of the procedures were performed by the resident physicians (73 out of 87 procedures); only 14 procedures were performed by a specialist or consultant. Majority of the EVD-related infection occurred in the group of cases performed by the resident group (26 out of 28 infected cases, 92.6%). There was no significant association (P = 0.21) between surgeon status and EVD-related infection. In this study, the venue for the procedure varied, although it was typically performed in the operation theatre (85 out of 87 procedures). Only 2 procedures were performed in the Intensive Care Unit (ICU) setting for ICP monitoring. We found that there was no significant correlation (P = 1.00) between the venue for the surgery and the risk of EVD-related infection. The majority of patients with EVD-related infections (26 out of 28 patients) presented with non-traumatic aetiologies. Cases of non-EVD-related infections were also more frequent among these patients with non-traumatic aetiologies (69.5%). It was found that there was no significant association (P = 0.16) between the traumatic and non-traumatic groups subjected to EVD with regard to the outcome of EVD-related infection. Therefore, EVD-related infection was independent of aetiology in this study. There were differences in terms of the duration of the EVD in situ among cases with different aetiologies. Patients with hypertensive-related aetiology subjected to EVD represented the largest subpopulation (18 patients, 20.7%), with duration of in situ EVD of more than 10 days. Multiple logistic regression analysis (Table 2) of controlled variables including sex, race, placement of the EVD, status of the surgeon, tunnelling length, and the duration of in situ EVD showed that EVD-related infection was significantly associated with both the length of tunnelling (P = 0.001) and the duration of in situ EVD (P = 0.024). EVD-related infection was noted to be 10 times less likely to develop in the group subjected to more than 5 cm of tunnelling. The EVD in situ of less than 10 days was noted to be 4 times less likely to develop EVD-related infection. Discussion The limited sample size in this study in comparison to the total number of patients subjected to EVD insertion and referred to the computed operation theatre database system, COTDS, (415 cases) results primarily from a high drop-off rate following the strict exclusion criteria. This prospective study included only patients with catheters constructed of similar material who had received only one EVD system. Traumatic patients who underwent parenchymal catheter insertion were also labelled as subjected to EVD insertion in the COTDS system, even though most of these patients did not undergo ventricular assessment for CSF sampling. Most patients with EVD had infected shunt systems and meningitis; these patients were excluded from the study. The overall incidence of EVD-related infection in patients with this EVD system has been reported to range from 0.0–21.9% of patients (1–11). However, various authors used different definitions of EVD-related infection, which may have either over- or under-estimated the true infection rate. Therefore, strict criteria based on literature review (13) were used to plan this study. The following categories were used to classify patients: infection, contamination, and colonisation. These strict definitions were created before the initiation of the study and the collection of data. The incidence of EVD-related infection at Hospital Kula Lumpur was found to be 32.2% (95% CI 23.3% to 42.6%), which is a relatively large fraction. This infection rate, as stated above, was obtained using strict inclusion and exclusion criteria; in particular, the system had to have been in situ for at least 48 hours before the patient could be included in this investigation. This minimum required duration of in situ catheterisation was meant to prevent misinterpretation of the results, as published studies have reported the infection to go undetected before day 3 of catheterisation (11,14). Most patients with traumatic head injury who required the EVD for ICP monitoring usually needed the system for only 48 hours. Furthermore, the measurement of tunnelling was performed at only day 3 of catheterisation to coincide with wound inspection and thereby avoid wound contamination during the study. Demographic data showed there was no significant difference for sex, race, or age in association with EVD-related infection. The majority of patients subjected to EVD insertion at HKL underwent surgery with catheter tunnelling of more than 5 cm. Tunnelling length has been found to be a significant risk factor for EVD-related infection; tunnelling of more than 5 cm length is associated with a lower rate of EVD-related infection. The use of 5 cm as the cut-off point is based on prior studies (15–17). Our findings are supported by another study (18), which noted no infection during the first 16 days of catheterisation when the extended tunnelling technique was used. Among 87 total samples, 60.8% of those with haemorrhagic-related disease, such as SAH or intracerebral haemorrhage, required an EVD. Previous research has documented a strong association between EVD-related infection and aetiological disease requiring an EVD. This is particularly prominent in cases of IVH and SAH (4,5,12). Previous studies have also shown a significant relationship between haemorrhagic CSF and EVD-related infection. This finding was consistent with our study, although the relationship was not significant. In cases of haemorrhagic-related diseases, the duration of in situ EVD is usually longer, which leads to an increased risk of drainage system blockage. The incidence of catheter blockage ranges from 19%–41% (6,19), which is why the catheter needs to be flushed and irrigated. A study by Aucoin et al. (10) noted a 24% infection rate in patients with flushed EVD systems, whereas Mayhall et al. (4) reported a higher incidence of EVD-related infection among those with catheter irrigation. In addition, the blood can act as a good medium for bacterial colonisation and subsequently promote infection (20). Patients were divided into 2 groups: those with duration of catheterisation of 10 days or less, and more than 10 days. The cut-off point was set at 10 days because published studies found a significant risk of EVD-related infection when catheterisation lasted for more than 10 days (1,7,21). Our findings are comparable with data from the literature (13), which reported an association between the duration of catheterisation and EVD-related infection. This study, as well as most others, demonstrated the lack of a significant association between the venue of EVD placement and EVD-related infection. However, the finding may be misleading because 85 of the patients in our sample (97.8%) underwent EVD insertion in the operation theatre. The same skewed distribution may colour conclusions related to the association between surgeon status and EVD-related infection because almost 83.9% of the EVD procedures were performed by a medical officer at our institution. Among the cases that have been classified as EVD-related infections in this study, Staphylococcus sp. and Acinetobacter sp. were most frequently isolated pathogen. Most of the bacteria isolated were Gram negative. Notably, a longer duration of EVD may facilitate microbial infection or colonisation. On the other hand, all patients subjected to EVD insertion were given a prophylactic dose of antibiotic to protect against contamination of the wound site by Gram-positive skin flora. Both the duration of EVD as well as the administration of antibiotic against Gram-positive bacteria may lead to subsequent infection by Gram-negative bacteria as opposed to the traditional Gram-positive flora. These findings are basically comparable to those observed by other authors, although some have noted a high rate of infection by Klebsiella sp. (22). This study has revealed that patients with haemorrhagic-related hydrocephalus with intraventricular extension will be managed with the EVD system in situ for more than 10 days. Such patients usually remain on the drainage system until the CSF system is conducive for a conversion to a permanent shunt. Researches have shown that patients who suffer from IVH will be dependent on the shunt system in about 55% of the cases (23,24). On the other hand, up to 63.4% of SAH patients will be shunt-dependent mainly due to communicating hydrocephalus (25–27). The CSF needs to be quite clean prior to shunt insertion, as post-haemorrhagic debris typically causes catheter or valve occlusion, especially in patients with IVH. However, not all patients need a permanent shunting system; a study revealed that up to 30% of IVH cases are resolved without evidence of hydrocephalus (28). This is probably due to the presence of blood products and associated inflammation in the cerebrospinal fluid. These factors dissipate with time, and once the cerebrospinal fluid is clear, hydrocephalus due to intracranial haemorrhage may resolve. Multivariate analysis comparing all the variables that can predispose patients to the risk of EVD-related infection showed that tunnelling length of more than 5 cm and catheterisation of 10 days and less can significantly reduce the incidence of infection. Conclusion Based on the findings reported here, subgaleal tunnelling of a catheter of more than 5 cm in length under the scalp is the recommended surgical technique, as this approach involves a significantly lower rate of EVD-related infection. A prolonged duration of catheterisation also plays an important role in relation to EVD-related infection, as it has been demonstrated that catheterisation of more than 10 days in duration is associated with a significant risk of developing EVD-related infection. Therefore, both subgaleal tunnelling of more than 5cm and 10 days and less of ventricular catheterisation should be implemented as standardised protocol at health institutions to reduce the risk of EVD-related infections. Authors’ Contributions Conception and design, final approval of the article: MAO, MSMH References
© Copyright 2010 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj10032t2.jpg] [mj10032t1.jpg] |
| |||||||||

{kind=link}
{kind=link}