 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
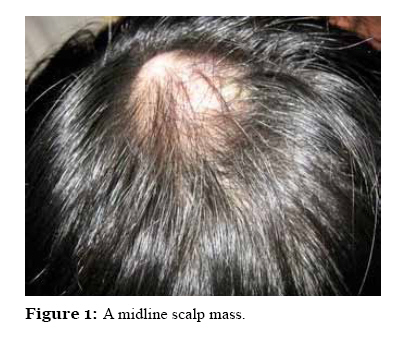
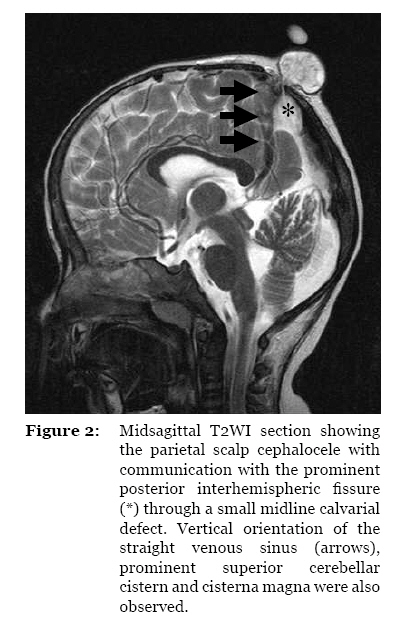
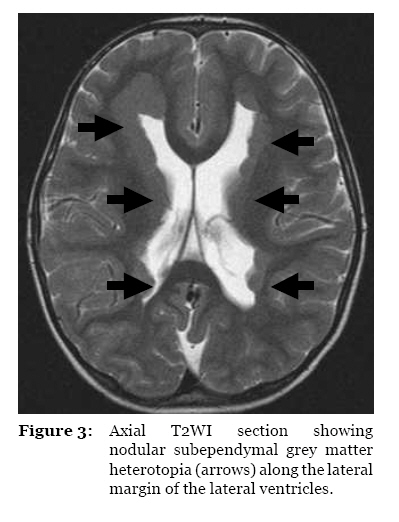
Malaysian Journal of Medical Sciences, Vol. 17, No. 3, 2010, pp. 61-63 Case Report Atretic Cephalocele — An Uncommon Cause of Cystic Scalp Mass Siong Lung Wong, Huong Ling Law, Suzet Tan Faculty of Medicine and Health Sciences, Universiti Malaysia Sarawak, Lot 77, Seksyen 22, KTLD, Jalan Tun Ahmad Zaidi Adruce, 93150 Kuching, Sarawak, Malaysia Correspondence: Dr Wong Siong Lung, MD (UKM), MMed (Radiology, UKM), Faculty of Medicine and Health Sciences, Universiti Malaysia Sarawak, Lot 77, Seksyen 22, KTLD, Jalan Tun Ahmad Zaidi Adruce, 93150 Kuching, Sarawak, Malaysia, Tel: +6082-416 550, Fax: +6082-422 564, Email: slwong@fmhs.unimas.my Submitted: 16 Aug 2009 Code Number: mj10034 Abstract A 6-year-old girl presented with a midline parietal scalp swelling that had been gradually enlarging since birth. Magnetic resonance imaging revealed communication of the cyst with the subarachnoid space through a calvarial defect, with concomitant findings of vertically positioned straight venous sinus and subependymal grey matter heterotopia. A diagnosis of atretic cephalocele was thus made based on these classical imaging findings. Keywords: cysts, encephalocele, scalp, magnetic resonance imaging, medical sciences Introduction Lumps and bumps in the scalp of a child are common presentations and may be difficult to diagnose because the differential diagnoses are very broad. Clinical examination alone is often inadequate for a final diagnosis. A good imaging strategy is required for proper diagnosis, particularly in cases with intracranial association. The possible causes of scalp lumps and bumps in a child include encephalocele, lipoma, sebaceous cyst, inclusion cyst, sinus pericranii, vascular lesion (e.g., haemangioma), tumours (e.g., Langerhans cell histiocytosis, fibrosarcoma, rhabdomyosarcoma, and metastatic disease), bone and soft tissue infection, and traumatic lesions (1). An accurate diagnosis is imperative in every case as it bears significant therapeutic implications. Case Report A 6-year-old girl with uneventful antenatal history presented with a painless midline scalp swelling over the parietal region starting in early infancy, with slow progressive enlargement of the swelling over the years. The parents expressed concern as the child had recently developed the habit of scratching the swelling, resulting in localised eczema. The child was otherwise asymptomatic with normal developmental milestones. There was no report of seizures. Physical examination showed a midline scalp mass that was cystic and non-mobile, measuring 3 x 4 cm in diameter (Figure 1). The scalp skin showed mild eczema and no discolouration. The hair overlying the swelling appeared sparse. The swelling was non-pulsatile and non-reducible. There was no bruit heard. Magnetic resonance imaging (MRI) revealed a parietal scalp cyst measuring 2.5 x 2.5 x 2 cm. There was a narrow cerebrospinal fluid (CSF) tract that connected the base of the cyst to the prominent posterior interhemispheric fissure through a small midline calvarial defect (Figure 2). No cerebral tissue was noted within the cyst. The straight venous sinus was nearly vertical in position and was observed just anterior to the CSF tract connecting the intracranial subarachnoid space to the scalp cyst. There was prominence of the superior cerebellar cistern and the cisterna magna. At the base of the scalp cyst, there was varicosity that drained into the superior sagittal venous sinus. Nodular subependymal grey matter heterotopia was noted along the lateral margin of the lateral ventricles (Figure 3). Midline structures, particularly the corpus callosum, were normal. Patient had the scalp cyst removed by the neurosurgeon and had an uneventful recovery thereafter. Discussion Atretic cephaloceles are small, skin-covered, subscalp lesions that contain meninges, neural rests, and glial rests. They are also known as atypical or rudimentary meningoceles, meningeal heterotopias, and meningoceles manqué. The development of atretic cephalocele has not been clearly elucidated. Atretic cephaloceles probably represent a manifestation of defects in closure of part of the neural tube (2). All previous reports of atretic cephalocele have been due to sporadic causes, with the exception of one series that reported three siblings having the same clinical diagnosis without any syndromic association (3). There is a wide range of clinical presentations of patients with atretic cephaloceles. A child may be normal with regard to neurodevelopmental milestones, or may have severe mental retardation if the atretic cephalocele is associated with severe intracranial anomalies, such as malformations of cortical development, Walker-Warburg syndrome, or ventriculomegaly (4). On examination, a small scalp nodule is palpable and generally covered with hairless scalp. In some cases, the cranial defect may be palpable. MRI is the best imaging modality to depict this entity. Upon imaging, an atretic cephalocele presents as a subscalp cyst with an associated calvarial defect at the vertex. Persistent vertical embryonic positioning of the straight sinus is seen in a majority of cases (4). There may be associated intracranial abnormalities, such as grey matter heterotopia, Walker–Warburg syndrome (with characteristic lissencephaly, hypoplasia of the metencephalon, and moderate to marked ventricular enlargement), lobar holoprosencephaly, Dandy–Walker syndrome, hypogenesis of the corpus callosum, extra-axial cysts, microphthalmia, and retro-ocular cysts (4,5). The prognosis of atretic cephalocele is generally good. Of the reported cases, only one case, which was associated with severe intracranial abnormalities (i.e., moderate hydrocephalus, lissencephaly, and metencephalic hypoplasia), showed profound psychomotor delay; the patient died at 3 years of age (4). Other reports of atretic cephalocele, even with associated with grey matter heterotopia, showed normal development as per the case presented herein. The treatment is surgical excision of the cyst and oversewing of the tract formed by the dura (5). Acknowledgements The authors wish to thank Mr Jensen and Mr Dennis, MRI radiographers at Sarawak General Hospital, for their technical assistance in writing this case report. Authors’ contributions Conception and design, collection and assembly of data, analysis and interpretation of data, drafting of article, final approval of the article: SLW References
© Copyright 2010 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj10034f3.jpg] [mj10034f1.jpg] [mj10034f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}