 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
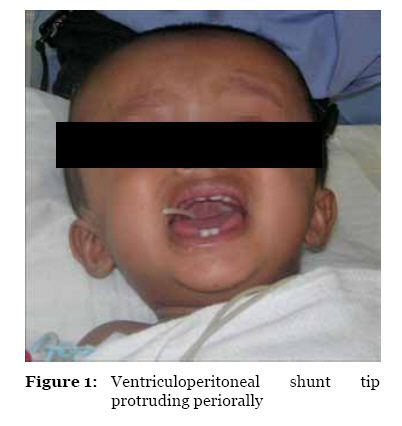
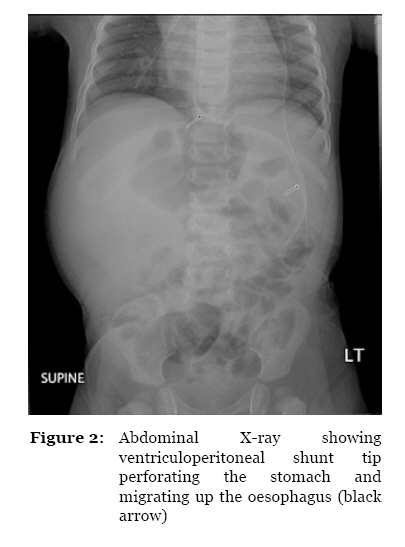
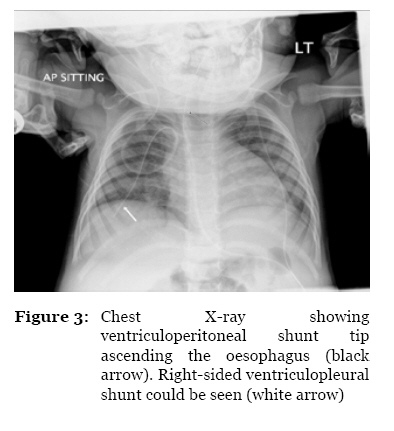
Malaysian Journal of Medical Sciences, Vol. 17, No. 3, 2010, pp. 64-67 Case Report Migration of the Abdominal Catheter of a Ventriculoperitoneal Shunt into the Mouth: A Rare Presentation Shiong Wen Low, Lwin Sein, Tseng Tsai Yeo, Ning Chou Division of Neurosurgery, Department of Surgery, National University Hospital, 5 Lower Kent Ridge Road, Singapore 119074 Correspondence: Dr Low Shiong Wen, MBBS, MRCSed, MMed (Surgery), Division of Neurosurgery, Department of Surgery, National University Hospital, 5 Lower Kent Ridge Road, Singapore 119074, Tel: +65-6779 5555 Hp: +65-9821 1118 Email: swlow@singnet.com.sg Submitted: 5 Nov 2009 Code Number: mj10035 Abstract A 1-year-old boy with a history of exomphalos and hydrocephalus had surgeries to correct these pathologies. The ventriculopleural (VPL) shunt inserted for hydrocephalus was complicated by pleural effusion, for which a ventriculoperitoneal (VP) shunt was inserted on the contralateral side. He subsequently presented with protrusion of the distal VP shunt tip from the mouth due to perforation through the gastrointestinal tract. The child also had a history of peritonitis post-exomphalos repair, which may have predisposed him to this relatively uncommon shunt complication. Probable causes and risk factors of the perforation are discussed. Keywords: foreign-body migration, in-dwelling catheters, intestinal perforation, post-operative complications, ventriculoperitoneal shunt, medical sciences Introduction Ventriculoperitoneal (VP) shunting is a common neurosurgical procedure for hydrocephalus. Rates of complications of VP shunts are widely reported, ranging 24%–47% (1), of which abdominal complications account for about 25% (2). Bowel perforation is reported to occur between 0.1% and 0.7% of the time (3–5) and may lead to significant morbidity and mortality as a result of peritonitis or meningoventriculitis. After bowel perforation, the catheter may present at one of the natural orifices, of which perianal protrusion is more common than perioral protrusion. We report a case of an infant who presented with perioral protrusion of the distal end of the VP shunt catheter as a delayed complication of the procedure. Probable causes, risk factors, and management principles are discussed. Case Report A 1-year-old boy was admitted to the neurosurgical unit after his mother noticed a tube coming out of his mouth after an episode of vomiting (Figure 1). He was a preterm baby born at 35 weeks of gestation via normal vaginal delivery with birth weight of 2936 grams. He had exomphalos major and was repaired at 20 hours of age by the paediatric surgical team. The repair was complicated by post-operative peritonitis, which was managed conservatively with parenteral antibiotics. He also had Haemophilus influenzae B meningitis complicated by hydrocephalus, for which a ventriculopleural (VPL) shunt was placed on the right side at one month of age. The decision to shunt the cerebrospinal fluid (CSF) to the pleural space was made due to the recent post-operative peritonitis. The VPL shunt was complicated by pleural effusion, and a VP shunt was inserted on the left side at the age of six months. The VPL shunt was ligated but not removed as we were uncertain if the VP shunt would function well with the possibility of adhesions from the previous peritonitis obstructing the peritoneal end of the VP shunt. The post-operative period was uneventful and the pleural effusion resolved spontaneously. The boy remained well until six months later, at 1 year of age, when he presented with protrusion of the distal end of the VP shunt through the mouth after an episode of vomiting. The child was afebrile and was clinically well and alert. There was no clinical evidence of meningitis or increased intracranial pressure (ICP). Examination of the abdomen did not reveal any signs of peritonitis. Chest and abdominal X-rays revealed that the peritoneal catheter had passed through the stomach and ascended up the oesophagus. There was no free gas under the diaphragm on the X-ray images (Figure 2 and 3). Intravenous vancomycin and ceftriaxone were started prior to the removal of the shunt and subsequent insertion of an external ventricular drain (EVD). We continued treatment with parenteral antibiotics and checked the CSF for leukocytosis and growth of organisms on the 14th post-operative day. There was no evidence of infection and the decision was made to reinsert a VP shunt on the left side. The operation and post-operative recovery was uneventful. The child was discharged well from our unit on the 7th post-operative day. The patient has been followed in the outpatient clinic since discharge. He has had regular follow-up for one year and has remained well with no complications related to the surgery. There were also no signs or symptoms of obstruction of the VP shunt. Discussion The VP shunt is the most widely used procedure in the treatment of hydrocephalus. As with any surgery, complications can occur. Although infrequent, abdominal complications have been reported. These include pseudocyst formation, intestinal obstruction, and bowel perforation and penetration (3). Most of these abdominal complications are delayed in occurrence. The incidence of bowel perforation by a shunt catheter is known to be low, occurring in 0.1%–0.7% of cases of complications (3–5). These complications can result in potentially fatal ventriculitis, meningitis, intraperitoneal abscess, faecal fistulae, peritonitis, or sepsis (6,7). There are at least 119 cases of catheter-induced gut perforations reported in the literature (5), with the colon being the most common site of perforation (70%), followed by the stomach (16%), and the small bowel (14%). It is postulated that the incidence of perforation is related to the mobility of the gut. The colon, being the most immobile, is the most frequently perforated viscus. The literature reviews (4,5) also revealed that, at all levels of perforation, the catheter was more likely to extrude through the anus (61.9%) or not at all (31.4%). Oral route protrusion was relatively uncommon as compared to anal extrusion, with a total of 10 cases reported in the literature (4,5,8–15). In this case report, the transoral presentation of the VP shunt catheter occurring six months after its insertion indicates delayed gut perforation. This complication was likely a result of a chronic process as opposed to an early bowel perforation that is usually due to direct injury or perforation during the shunting procedure itself. Delayed gut perforation has been found to be associated with young age, male gender, malnutrition, silicon allergy, length of catheter, previous abdominal surgery, and infection (9,13). Age seemed to be the main risk factor for bowel perforation. It was postulated that, in children, their weaker intestinal musculature and stronger intestinal peristaltic activity result in higher incidence of bowel perforation (4). The catheter tip causes a chronic irritative process to the serosal surface of the bowel wall and subsequently leading to repeated pressure and inflammation, and eventual ulceration and perforation. Our patient is a male and presented at one year of age with a history of peritonitis after abdominal surgery for exomphalos major. Furthermore, the distal length of the peritoneal catheter that was placed in the peritoneal cavity was about 20 cm, and it was inserted into the left hypochondrium. The previous peritoneal infection and adhesions together with the long distal length of the VP shunt contributed to the pressure necrosis of his stomach wall. We postulated that this eventually resulted in the penetration and subsequent fibrotic wall formation along the perforated site of the peritoneal cavity. As such, the child did not present with signs of peritonitis or gas under the diaphragm in the abdominal X-ray. The tube seemed to have penetrated the stomach wall and then ascended along the oesophagus and protruded out of the mouth during the child’s forceful emesis. Diagnosis of shunt perforation of the bowel may not be obvious if the shunt catheter does not protrude through the natural orifices (13), and patients do not always present with significant abdominal symptoms (16), as in the patient in this case report. This fact is because the fibrous tract formed at the perforated site usually seals the perforation, preventing spillage of faecal matter into the peritoneum, which would otherwise lead to peritonitis. Hence, the correct diagnosis may be delayed until a later stage at which ventriculitis or central nervous system (CNS) infection has been fully established, leading to significant morbidity and/or mortality. Radiologic investigations, such as plain X-ray and contrast CT, are useful in cases when the diagnosis of bowel perforation is suspected. The management principles of such VP shunt complications include removal of extruding shunt tubing, attention to the perforated viscus, and treatment of possible peritonitis and/or meningoventriculitis. For this patient, we removed the extruding shunt though the oral orifice after the removal of the shunt valve and ventricular catheter through the cephalic incision. There was no need for exploratory laparotomy as the child did not show any signs or symptoms of peritonitis. Intravenous antibiotics were given for 14 days before reinsertion of the VP shunt as per our hospital protocol, although the duration may not need to be this lengthy as no clinical signs of meningitis or ventriculitis were noted. In conclusion, the appearance of the tube in the mouth represented bowel penetration. Spontaneous bowel penetration or perforation is a rare complication of VP shunt surgery. A high index of suspicion is essential, particularly in paediatric patients, to diagnose perforation or penetration as the abdominal signs and symptoms may be vague (16). Abdominal radiology, including plain X-ray and contrast CT, may be required in some cases (5). CSF culture is also mandatory for diagnosis of retrograde CSF infection to ensure early and appropriate antibiotic treatment. Early removal of the suspected shunt and conversion to external ventricular drain for CSF diversion are important measures for control of CNS infection. The selection of a clean site for CSF diversion is imperative for successful management of complicated paediatric cases. Authors’ Contributions Conception and design, provision of study materials or patients, collection and assembly of data, analysis and interpretation of data, drafting of article: SWL, LS References
© Copyright 2010 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj10035f3.jpg] [mj10035f2.jpg] [mj10035f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}