 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
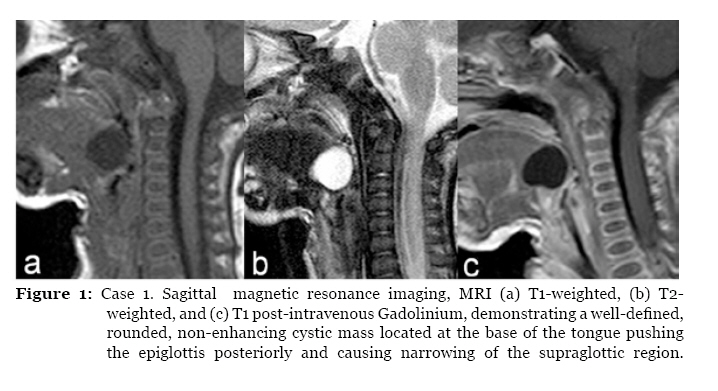
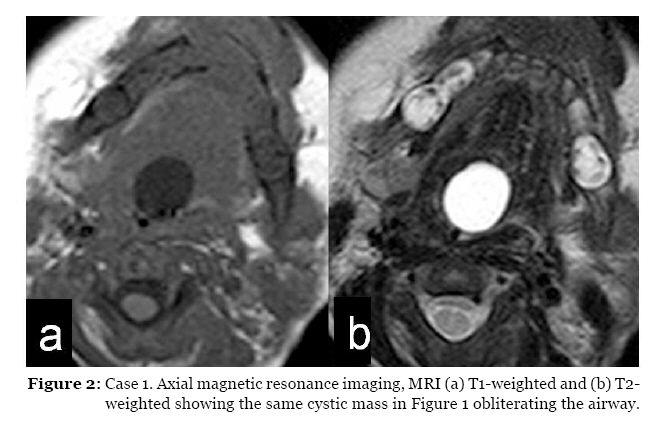
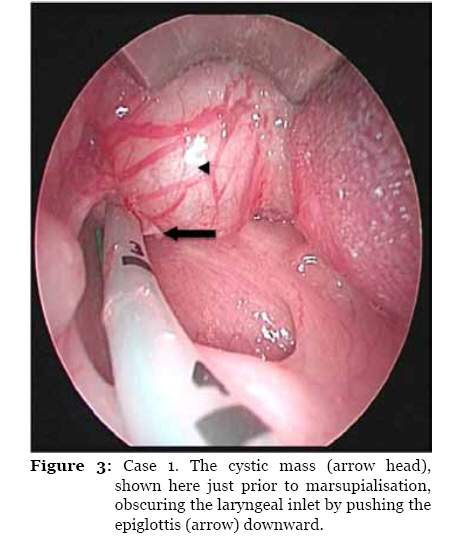
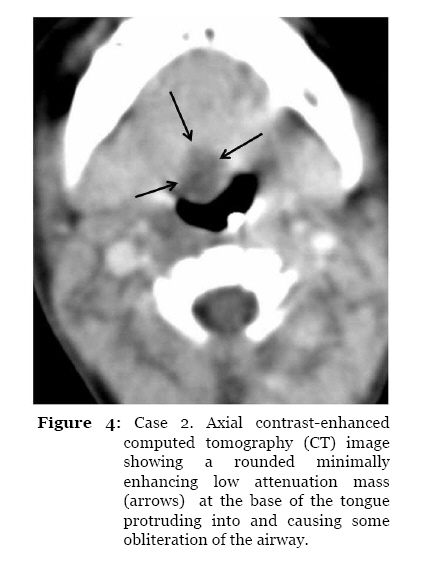
Malaysian Journal of Medical Sciences, Vol. 17, No. 3, 2010, pp. 68-73 Case Report Two Cases of Congenital Vallecular Cyst: A Reminder of the Potentially Fatal Cause of Upper Airway Obstruction in Infants Azian Abd. Aziz1, Ahmad Fadzil Abdullah2, Raja Ahmad Rl Ahmad3 1Department of Radiology, Kulliyyah of Medicine, International Islamic University Malaysia, 25200 Kuantan, Pahang, Malaysia Correspondence: Dr Azian Abd Aziz, MD, MMed (Radiology), Department of Radiology, Kulliyyah of Medicine, International Islamic University Malaysia, 25200 Kuantan, Pahang, Malaysia, Tel: +6012-9086324 Fax: +609-5177631 Email: drazianaziz@gmail.com Submitted: 19 Dec 2009 Code Number: mj10036 Abstract Vallecular cyst, a benign yet rare laryngeal lesion, may cause stridor and even life-threatening upper airway obstruction in infants. It can cause apnoea and poor feeding habits, thus reducing the chance of survival. Although laryngomalacia remains the most common cause of stridor in this age group, awareness and a high level of suspicion for this condition can help lead to early management and intervention. Direct laryngoscopy is accepted as the gold standard for diagnostic purposes, and marsupialisation of the cyst is the preferred treatment. We describe 2 cases of vallecular cysts in infants admitted to our hospital where timely diagnoses led to appropriate treatment. Keywords: cyst, infant, laryngoscopy, magnetic resonance imaging, stridor, medical sciences Introduction A vallecular cyst is a rare type of laryngeal cyst seen in infants. Stridor with or without respiratory distress is the most common presentation secondary to narrowing of the airway. Even though there have been many cases reported in the literature, we strongly believe that medical officers in district hospitals or even smaller clinics, including paediatricians and general practitioners, need to be repeatedly reminded and made aware that this condition exists so that it can be quickly identified and affected children can be managed promptly and appropriately. Here, we describe 2 cases of vallecular cysts seen within a 1-year period in our hospital. In both cases, patients were initially seen by a general practitioner and then a medical officer in a district hospital—the typical scenario for vallecular cyst patients, which highlights the importance for every medical professionals and clinicians to recognize and be reminded of this lesion. Case 1 A 2-month-old baby girl was referred to us for noisy breathing and progressive respiratory distress. She was born at term by vaginal delivery with an uneventful neonatal period. Noisy breathing was noted by her parents a few days after birth and continued to worsen; 2 days prior to the referral, she had increasingly noisy breathing, respiratory distress, and refused to feed. The baby was brought to a general practitioner, who then referred her to the hospital. Upon examination, her vital signs were stable and there were no dysmorphic features. She was in respiratory distress with marked inspiratory stridor, and she was also tachypnoeic with suprasternal and subcostal recession that improved slightly with oxygen supplementation. The lung air entry was decreased bilaterally. Other systems were unremarkable. Laboratory results were normal. An initial diagnosis of severe laryngomalacia was made. A flexible upper airway scope showed a cystic mass at the base of the tongue. Urgent direct laryngoscopy under general anaesthesia (GA) confirmed the cystic mass at the base of the tongue, which was pushing the epiglottis against the posterior pharyngeal wall and obstructing the laryngeal inlet. The aryepiglottic folds were short with the presence of redundant mucosa over the arytenoids. An emergency tracheostomy was performed to view the upper airway obstruction and allow further radiological characterisation of the mass prior to a definitive surgery. Magnetic resonance imaging (MRI) of the neck, performed once the baby’s condition had been stabilised, showed a well-defined, non-enhancing, fluid-filled mass located at the base of the tongue, measuring approximately 1.5 x 1.3 cm in size (Figures 1 and 2). The airway was narrowed while the epiglottis was obliterated. Based on the MRI findings, differential diagnosis of a thyroglossal duct cyst or a vallecular cyst was made. Marsupialisation of the cystic mass (Figure 3) and bilateral laser aryepiglottoplasty were subsequently performed. The cyst contained a clear mucoid secretion. The tracheostomy tube was decannulated a week later. A final diagnosis of a vallecular cyst was made based on the operative and MRI findings. The stridor markedly improved and the baby had an uneventful recovery. At the 3-month follow-up examination, the child was thriving well with no evidence of stridor. A flexible pharyngoscopy showed no evidence of cyst recurrence, and the laryngeal inlet was well-visualized. Case 2 A previously well, term 3-month-old baby boy was referred to our hospital for progressive difficulty in breathing. He was asymptomatic until he developed stridor and progressive respiratory distress from 2 months old. He was initially brought to a district hospital and was noted to be cyanosed upon examination and required intubation. He was then treated as having bronchopneumonia and was extubated a few days later. A flexible upper airway scope revealed a cystic lesion in the supraglottic area. He was then referred to our hospital for further management. Upon examination in our hospital, he was not dysmorphic and his vital signs were stable. We also observed inspiratory stridor as well as suprasternal and subcostal recession. The air entry was decreased in both lungs. Other systems were normal. Laboratory results were also normal. A diagnostic direct laryngoscopy under GA demonstrated a cystic mass adherent to the base of the tongue and vallecula. The epiglottis was compressed posteriorly and the laryngeal inlet was obscured. The aryepiglottic folds were short. The vocal cord and subglottic region were normal. An emergency tracheostomy was done in view of the impending airway obstruction. A computed tomography (CT) scan showed a rounded, hypodense lesion at the base of the tongue measuring approximately 1.2 x 1.1 cm in size, which was causing obliteration of the airway (Figure 4). Minimal enhancement of this lesion was noted post-intravenous contrast. Marsupialisation of the vallecular cyst was performed, and the cyst contained a clear fluid. A repeat flexible upper airway scope 1 week later revealed reaccumulation of the cyst with collapsed epiglottis. The previous incision was reopened under GA, and this time, the aryepiglottic folds were released with a laser. The laryngeal inlet was observed, and no recurrence of the cyst was seen in the subsequent repetition of upper airway scope. Discussion The 2 cases described in this article illustrate that even a mass that is small in size, located within the larynx of infants and younger children, has the potential to cause significant upper airway obstruction because of the relatively small airway. Such a condition may be fatal if not clinically identified. Inspiratory stridor, which was observed in both our patients, is an important clinical finding or symptom and usually indicates a lesion arising from the supra- glottis and glottis region. Therefore, the underlying cause must be determined. The stridor occurs due to a “ball–valve” effect caused by the obstructing lesion or mass. The most usual cause of inspiratory stridor and supralaryngeal airway obstruction in infancy is laryngomalacia (1–3). Another clinical manifestation that may develop in the presence of a laryngeal lesion is repeated apnoea. Unless there are alarming symptoms or signs of respiratory distress from upper airway obstruction, diagnosis of a laryngeal lesion may be delayed, and appropriate treatment may not be achieved in a timely manner. Differential diagnosis of a lesion that may cause airway obstruction in this region would include haemangioma, vascular malformation, thyroglossal duct cyst, dermoid cyst, brachial cleft cyst, congenital ranula, and even alimentary tract duplication (4,5). Laryngeal cysts represent a collection of benign laryngeal abnormalities and classifications that have been reported based on their histologic appearances, size, contents, or localisation within the larynx (6). Aryepiglottic cysts represent the most common laryngeal cysts in children (4,7). Laryngeal cysts located in the vallecular space, as seen in our patients, are thus called vallecular cysts. This entity is a rare but known cause of congenital stridor, respiratory distress, and airway obstruction in infants (3,5,8). It can also cause interrupted feeding due to distress that may lead to failure to thrive (1,7,8). The vallecular cyst is a unilocular cystic mass of variable size that arises from the lingual surface of the epiglottis and usually contains clear, non-infected fluid (7,9). It is a ductal type of laryngeal cyst, which arises from fluid accumulation secondary to obstructed submucosal glands. The other type is a saccular cyst, which is submucosal cyst caused by mucous accumulation within the laryngeal saccule (2). When a laryngeal lesion is suspected, visualisation by direct laryngoscopy is the main investigative tool in the diagnosis of a vallecular cyst, as the presence of the lesion can be confirmed and the degree of airway compromise can be assessed. Imaging modalities such as CT or MRI are useful, as they can provide information concerning the nature and extent of the lesion, particularly in the pre-operative setting. Although the lesions were already seen via endoscopy in both of our cases, further radiological imaging was required preoperatively to confirm their cystic nature, assess the vascularity of the lesions, and determine their actual sizes. CT or MRI can explicitly demonstrate the relationship of the lesion with surrounding structures, particularly the neurovascular structure, which is helpful during surgical exploration. Large lesions may obliterate or displace adjacent structures. CT of most cystic masses will show similar low-density attenuation. Using MRI analysis, a vallecular cyst will appear hypointense on T1, hyperintense on T2, and does not enhance following intravenous Gadolinium. Although ultrasound can provide information about the structure, location, and vascularity of the lesion, further evaluation with CT or MRI is useful for the aforementioned reasons. A vallecular cyst suspected during antenatal ultrasound and diagnosed with fetal MRI has been previously reported (4). Prenatal detection of this condition allows appropriate counselling and planned preparation for intervention. For example, an emergency tracheostomy may be warranted upon delivery when oral intubation is impossible or, in some centres, where the ex-utero intrapartum treatment (EXIT) procedure is performed. Awareness and a high level of suspicion are required for a quick diagnosis of a laryngeal lesion or, as in our cases, vallecular cysts. Laryngeal lesion can be suspected from a thorough history and physical examination, especially when an infant presents with a congenital stridor. Imaging with MRI or CT would be helpful pre-operatively to further characterize the lesion. Direct laryngoscopy remains the major diagnostic tool for a definitive diagnosis. Surgical excision of the cyst is the treatment of choice and, when performed in a timely manner, gives a good prognosis. Acknowledgement The authors would like to thank the Director General of Health, Ministry of Health of Malaysia and the Hospital Director, Hospital Tengku Ampuan Afzan, Kuantan, Pahang, Malaysia for permitting the publication of these 2 cases. Authors’ Contributions Conception and design, drafting of the article, final approval of the article, administrative, technical, or logistic support: AAA References
© Copyright 2010 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj10036f1.jpg] [mj10036f4.jpg] [mj10036f3.jpg] [mj10036f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}