 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
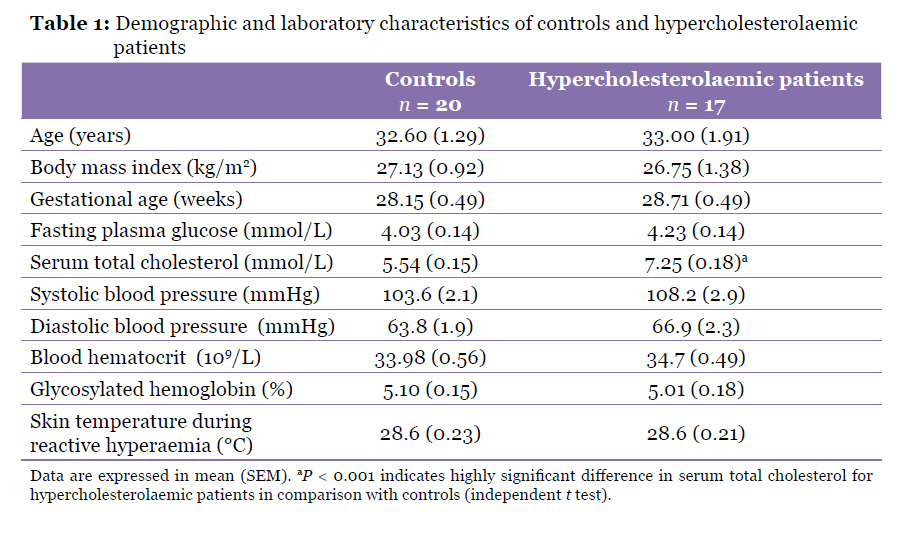
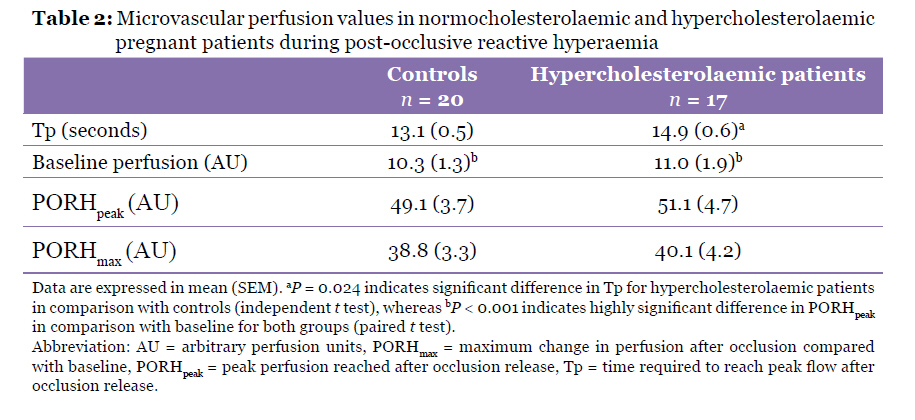
Malaysian Journal of Medical Sciences, Vol. 17, No. 3, 2010, pp. 14-19 Original Article Abnormal Microvascular Reactivity with Hypercholesterolaemia in Pregnancy Aida Hanum Ghulam Rasool1, Aisyah Syairah Abdul Rahman1, Nor Aliza Abd Ghaffar2, Nik Mohd Zaki Nik Mahmood2, Abd Rahim Wong3 1Pharmacology Vascular Laboratory, School of Medical Sciences, Universiti Sains Malaysia Health Campus, 16150 Kubang Kerian, Kelantan, Malaysia Correspondence: Associate Professor Dr Aida Hanum Ghulam Rasool, MBBS (Flinders), PhD Clinical Pharmacology (USM), School of Medical Sciences, Universiti Sains Malaysia Health Campus, 16150 Kubang Kerian Kelantan, Malaysia, Tel: +609-7676123 / 6143 Fax: +609-7653370 Email: aida@kb.usm.my Submitted: 12 Jan 2010 Code Number: mj10042 Abstract Background: Post-occlusive skin reactive hyperaemia (PORH) is a model used to assess microvascular reactivity. This study aims to compare PORH response among pregnant hypercholesterolaemic patients with age and gestational age-matched controls. Keywords: hypercholesterolaemia, laser Doppler flowmetry, microcirculation, pregnancy, reactive hyperaemia Introduction Hypercholesterolaemia is an important cardiovascular risk factor and a potent factor contributing to the progression of atherosclerosis (1). It is associated with endothelial dysfunction and reduced endothelium-dependent responses in the forearm and coronary circulation (2,3). Maternal hypercholesterolaemia during pregnancy has been reported to be associated with enhanced fatty streak formation in human foetuses (4). The hypercholesterolaemic condition during pregnancy may also modify vascular and placental functions, contributing to complications during pregnancy or to the offspring. It has been shown that pregnant rats fed a diet enriched in cholesterol showed 4-fold increase in abortions, 2-fold increase in neonatal mortality, smaller litter size, and a lower birth weight of pups (5). Post-occlusive skin reactive hyperaemia (PORH) is the increased of blood flow after temporary occlusion of the arterial blood flow. The hyperaemic response to an ischaemic block is thought to be endothelium-dependent, involving myogenic response and release of metabolic factors such as nitric oxide (NO) and prostaglandins. Assessment of PORH by laser Doppler fluximetry (LDF) is a simple, non-invasive and reproducible method to assess microvascular health (6,7). Besides providing information on baseline blood flow measurements, the time-course of the cutaneous response to post-ischaemic reactive hyperaemia can give information on changes occurring in the microcirculation (8). Cutaneous post-ischaemic reactive hyperaemia has been used to detect microvascular reactivity differences between smokers and non-smokers (9), diabetic patients and controls, as well as between subgroups of diabetic patients (10). More recently, post-hyperaemia flux was reported to be significantly lower, and time to achieve peak post-ischaemic response was slower in diabetics compared with controls (11). Farkas et al. have demonstrated that hypertensive patients have a lower maximal change in skin blood flow with reactive hyperaemia compared with controls (12). Normal pregnancy is characterized by reduced peripheral vascular resistance and blood pressure, increased cardiac ouTput, and subsequent increase of blood flow in the systemic and pulmonary circulations. Brachial artery flow-mediated dilatation was found to be increased from the first trimester, reaching the highest value in the last trimester compared with non-pregnant values. However, no studies have directly compared microvascular or skin vascular reactivity using reactive hyperaemia method between healthy non-pregnant and pregnant women. In pregnant women, vascular reactivity has been shown to be altered in skin vessels of pre-eclamptic patients (13). In normotensive pregnant subjects, the reactive hyperaemia response was nearly as pronounced as the maximal vasodilatation of the vessels induced by local heating. However, in patients with pre-eclampsia, the reactive hyperaemia response reached was only half of the maximal vasodilatory capacity. Pre-eclamptic women were also shown to have lower post-occlusive reperfusion compared with controls, besides having lower basal blood flow (14). Dyslipidemia has been shown to impair microvascular reactivity in non-pregnant subjects (7,8,15,16). The effect of hypercholesterolaemia on the microvascular bed has not been studied in pregnant women. It is not known whether the difference in reactivity between normocholesterolaemic and hypercholesterolaemic patients persists in the presence of altered cardiovascular, hormonal, and metabolic adaptations occurring during pregnancy. Thus, this study aims to compare microvascular reactivity between pregnant women with hypercholesterolaemia and age-matched as well as gestational age-matched controls. LDF and the PORH response were used to assess microvascular reactivity in these women. Materials and Methods SubjectsThis prospective, cross sectional study involved 17 pregnant hypercholesterolaemic patients and 20 age and gestational-aged matched women. Ethical approval for the conduct of this study was obtained from the Ethical Committee of Universiti Sains Malaysia. This study was conducted following the principles stated in the Declaration of Helsinki; all subjects voluntarily signed an informed consent form. Subjects were recruited from the Obstetrics and Gynaecological Clinic of Hospital Universiti Sains Malaysia when they presented between 25–33 weeks gestation. Pregnant women with significant cardiovascular diseases (such as hypertension, arrhythmia, and heart failure), diabetes mellitus, history of previous and current gestational diabetes, multiple pregnancies, foetal anomalies, and serious maternal illnesses (such as liver and renal diseases) were excluded. All subjects underwent a modified oral glucose tolerance test (MOGTT) to exclude gestational diabetes. None of the subjects were taking any vasoactive medication such as non-steroidal anti- inflammatory drugs, corticosteroids, or lipid-lowering drugs. Women were categorized into the hypercholesterolaemic group if their serum total cholesterol (TC) was equal to or more than 6.5 mmol/L. At this cholesterol level, the risk of developing coronary artery disease is substantially increased (17). LDF and PORH responseThe LDF DRT4 system (Moor Instruments, Axminster, UK) was used in this study to non-invasively measure the forearm skin blood perfusion. This equipment was used together with the DP1T-V2 skin laser probe (Moor Instruments, Axminster, UK). LDF of skin blood flow is based on measurement of the Doppler shift principle wherein photons of laser light are scattered by moving blood cells to produce a Doppler shift on the reflected light. The outcome is generally termed as ‘flux’ and expressed in arbitrary perfusion units (AU). Laser Doppler measurements on the pregnant women were carried out in the morning in a quite room with room temperature maintained at 23 (SD 1) °C. Upon arriving, subjects lay down for at least 15 minutes for acclimatization before their blood pressure was taken using an automated blood pressure sphygmomanometer (Omron, Japan).The right arm of the subject was placed on a cushion and supported by a hand supporter to reduce involuntary hand movements. A sphygmomanometer cuff (Accoson, UK) was placed around the right upper arm 1–2 cm above the ante-cubital crease. Laser Doppler probes were then fixed on the volar surface of the right forearm distal to the sphygmomanometer occlusion cuff. After a stable skin perfusion was obtained, baseline skin perfusion flux was recorded for 1 minute. Forearm blood flow was then performed by inflating the pneumatic pressure cuff placed on the right upper arm to a supra- systolic pressure of 200 mmHg for 3 minutes. After 3 minutes, the occlusion cuff was rapidly deflated and perfusion flux was recorded for at least 2 minutes. Both the skin perfusion and temperature were measured continuously before, during and after occlusion by the laser Doppler probes. Skin perfusion was allowed to return to baseline; an interval of at least 15 minutes (or until baseline flux was achieved, whichever was longer) was allowed before a repeat of the procedure. The following parameters were measured: minimum baseline perfusion, the time required to reach peak flow after occlusion release (Tp), peak perfusion reached after occlusion release (PORHpeak), and maximum change in perfusion after occlusion compared with baseline (PORHmax) which was calculated as PORHpeak minus minimum baseline perfusion. The average of 2 readings for each parameter was recorded. A single operator was responsible for performing the reactive hyperaemia procedure throughout this study to reduce inter-operator variability. The intraday and interday coefficient of variations for PORHmax and Tp at our laboratory was 4.77% and 6.5%, and 8.89 and 6.87%, respectively (6). Blood sample for the measurement of serum TC was taken after an overnight fast. Serum TC was measured at the Chemical Pathology Laboratory, Hospital Universiti Sains Malaysia, using commercially prepared reagents (Enzymatique Endpoint, Randox) on the Hitachi Model 902 auto-analyser (Japan). The within and between run coefficient of variation for determining serum TC at the laboratory was less than 2%. Statistical analysis was performed using the SPSS version 12 (SPSS Inc., Chicago, IL). Results are presented as mean and SEM; P < 0.05 defined statistical significance. Differences between groups were evaluated using the independent t test or Mann–Whitney U test, where applicable. Results Mean age and gestational age for the subjects were 32.8 (SEM 1.1) years (ranged 21–45 years) and 28.4 (SEM 0.3) weeks (ranged 25–33 weeks), respectively. Baseline characteristics for the controls and hypercholesterolaemic patients are shown in Table 1. Apart from the serum TC values, there were no significant differences between the controls and hypercholesterolaemic subjects in their age, gestational age, blood pressure, blood count values, body mass index, and fasting plasma glucose values. There was also no significant difference in their skin temperature during the PORH procedure. Arterial occlusion induced by the occlusion cuff around the upper arm and inflated to 200 mmHg for 3 minutes resulted in a significantly lower perfusion recording compared with baseline. After occlusion release, the blood flow increased rapidly to a peak value approximately 5-fold compared with baseline; but the perfusion decreased again towards baseline soon after. Both groups showed significant increases in PORHpeak compared with baseline (P < 0.001 in both groups). Baseline perfusion, Tp, PORHpeak, and PORHmax for the normocholesterolaemic and hypercholesterolaemic groups are shown in Table 2. There were no significant differences between the 2 groups in baseline perfusion, PORHpeak, and PORHmax. There was however, significant difference between the 2 groups for Tp; the hypercholesterolaemic group showed significantly longer Tp compared with the controls. Linear regression analysis was performed to assess the relationship between serum TC and Tp. There was a positive significant correlation (P = 0.015, r = 0.4) between the 2 parameters; higher serum TC values were associated with longer Tp. Discussion We found that the presence of hypercholesterolaemia in pregnancy prolonged the Tp with the process of PORH compared with the age and gestational age-matched controls. Microvascular reactivity among non-pregnant, hypercholesterolaemic subjects has been reported in the literature (7,8,16,18). Binggeli et al. reported that post-ischaemic skin blood flow measured using the LDF was markedly reduced in hypercholesterolaemic patients compared with healthy controls and statin improved the post-ischaemic hyperaemia in the subjects after an average of 6 months of treatment (7). Unlike the study by Binggeli et al., no difference in peak hyperaemic response was seen in our study. Two possible reasons may explain this difference; firstly, the mean age of our subjects was 33 years compared with theirs, which was 42 years. It is possible that older subjects experience more vascular function abnormality with hypercholesterolaemia compared with the younger age group. The older age group may also have been exposed to a longer duration of high lipid levels. Secondly, our subjects were all female and pregnant, whereas in their study, 17 out of 19 subjects were males and there were no pregnant women. Most of their subjects were also on other drugs, mostly cardiovascular-related, such as acetyl salicylic acid, antihypertensives, and diuretics, indicating that some of these patients may already had some vascular/endothelial dysfunction present. In the study by Binggeli et al., Tp achieved by each group was not reported. Stulc et al. have observed that microvascular reactivity in hypercholesterolaemic patients without coronary artery disease was not different from controls. Microvascular reactivity was, however, reduced in hypercholesterolaemic patients with coronary artery disease (16). Patients with hypertriglyceridemia were reported by Tur et al. to show cutaneous microcirculatory changes in the forearm. Untreated hypertriglyceridemic patients have significantly lower peak flow compared with controls and patients treated with the lipid-lowering drug, bezafibrate (8). The hyperaemic reaction was also faster in the bezafibrate-treated group compared with the other 2 groups. Apart from our current study, there are no studies assessing the effect of hypercholesterolaemia on microvascular reactivity in pregnancy. Haak et al. reported that Tp during PORH was shorter in hyperlipidaemic patients after treatment with the statin fluvastatin; this was associated with a 22.8% reduction in serum TC level (18). Gomes et al. reported that Type 1 diabetic patients took longer to reach peak flux during hyperaemia response compared with age-matched controls (19). The mean age of their subjects was 33 years. Similar to our study, no difference in PORHmax was observed between the 2 groups (19). Similarly, Tur et al. had demonstrated that in diabetic patients, PORHpeak was lower than non-diabetic controls; diabetics also had longer Tp compared with controls (10). There are a few possible mechanisms whereby hypercholesterolaemia contributes to prolonged Tp. Functional or a combination of functional with structural vascular changes might produce these microvascular abnormalities. Firstly, elevated serum TC may increase blood viscosity and increase the Tp. Secondly, there may be failure of prompt vasodilatation by smooth muscle cells in response to ischemia in hypercholesterolaemic subjects. During reactive hyperaemia, ischaemic stimulation forces the endothelium to release vasodilating substances such as NO and prostaglandins. In normal subjects, the response to occlusion and release would be fast and efficient, but in hypercholesterolaemia, the endothelium may take a longer time to respond, causing a longer time for reperfusion. This may be due to impairment in the diffusion of NO into the smooth muscle of the vessel wall. Hypercholesterolaemia has been reported to impair endothelium-dependent relaxation in the microcirculation and macrocirculation in experimental animals and humans (20,21). This may be due to reduced synthesis of endothelium-derived relaxing factors, or altered membrane receptor coupling mechanisms that affected the release of these factors. Since NO normally interferes with the action and synthesis of endothelin (an endogenous vasoconstrictor), the lack of NO activity may favour the vascular expression of endothelin. Thirdly, hypercholesterolaemia may cause a reduction in vasodilating substances produced by the endothelium by creating a condition of oxidative stress. Free radicals, such as superoxide anion, have been known to scavenge endothelium-derived relaxing factor (22). Lastly, structural changes in the blood vessel, such as wall thickening, may also reduce the speed of response to ischaemia. The primary limitation of this study in that only the serum TC value was available, while the detailed lipoprotein results were not. However, the results from this study will hopefully form the basis for more detailed study in this area. Another limitation of this study is that the duration of hypercholesterolaemia in these patients is unknown; some women may be more relaxed in their dietary habits during pregnancy. However, the strength of this study is that, apart from the serum TC values, there was little difference in characteristics of the controls and the hypercholesterolaemic subjects, wherein both groups were screened for impaired glucose tolerance, they were not on any vasoactive drugs, none of the hypercholesterolaemic subjects had ever been treated with lipid lowering agents, and neither group had any cardiovascular diseases. Conclusion We conclude that hypercholesterolaemia in pregnancy affects microvascular reactivity by increasing the time needed to achieve peak perfusion after temporary arterial occlusion. More detailed study in this population correlating detailed lipid profile, microvascular reactivity, placenta blood flow, and pregnancy outcome is suggested. Acknowledgement We thank Universiti Sains Malaysia for providing financial assistance to conduct this study (grant no: 304/PPSP/6131501). Authors’ contributions Conception and design, obtaining of funding, critical revision and final approval of the article: AHGR, NAAG, NMZNM, ARW References
© Copyright 2010 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj10043t2.jpg] [mj10043t1.jpg] |
| |||||||||

{kind=link}
{kind=link}