 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 17, No. 3, 2010, pp. 36-43 Original Article Risk Factors and Phenytoin Prophylaxis for Early Post-Traumatic Seizures among Patients with Traumatic Brain Injury Chan Kin Hup1, John Tharakan2, Hillol Kanti Pal2, Naeem Khan3, Tan Yew Chin2 1Department of Surgery, Kulliyyah of Medicine, International Islamic University Malaysia, Jalan Istana Bandar Indera Mahkota, 25200 Kuantan, Pahang, Malaysia Correspondence: Dr Chan Kin Hup, MMed Neurosurgery (USM), Department of Surgery, Kulliyyah of Medicine, International Islamic University Malaysia, Jalan Istana Bandar Indera Mahkota, 25200 Kuantan, Pahang, Malaysia, Tel: 09-571 6770 Email: khchan@hotmail.com Submitted: 21 Oct 2009 Code Number: mj10046 Abstract Background: Post-traumatic seizure is a well-known and serious complication of traumatic brain injury (TBI). The incidence and risk factors vary among study populations. Very little data have been published concerning this in the Malaysian population. The aim of this study was to ascertain the risk factors for the development of early post-traumatic seizures among patients with TBI. Keywords: Post-traumatic epilepsy, traumatic brain injury, head injuries, incidence, risk factors, phenytoin Introduction Traumatic brain injury (TBI) poses a major health and socioeconomic problem throughout the world today (1). One of the important but poorly understood sequelae of TBI is post-traumatic seizures. Post-traumatic seizures can happen either early (occurring within 1 week of the injury) or late (occurring from 1 week to years after the injury). Recurring late seizures make up the clinical syndrome of post-traumatic epilepsy (2–4). The significance of an early post-traumatic seizure lies in the fact that a seizure attack within the acute stage may result in cerebral hypoxia, increased intracranial pressure (ICP) and metabolic demand, an increased release of neurotransmitters, and, thereby, a higher incidence of mortality and morbidity due to secondary brain damage (5,6). Reported risk factors for the development of seizures in the first week after injury include acute intracerebral haematoma (especially subdural haematoma), younger age, increased severity of injury and chronic alcoholism (4). Although early post-traumatic seizure is an important sequelae of TBI with potentially deleterious effects to life and recovery, to date, there are very little data concerning incidence and risk factors among the local population. Ong et al. (7) reported an incidence of 5.5% of early seizures in the paediatric population of the Kuala Lumpur General Hospital. The objectives of this study were to determine the incidence and the relevant clinical and patient-related parameters that may contribute to the time in the development of early post-traumatic seizures. Materials and Methods This was a prospective observational study carried out in Hospital Universiti Sains Malaysia (HUSM), Kubang Kerian, Kelantan, Malaysia. The study participants were patients who were admitted with a diagnosis of head injury from June 2007 to November 2007, except for those who met any of the following exclusion criteria:
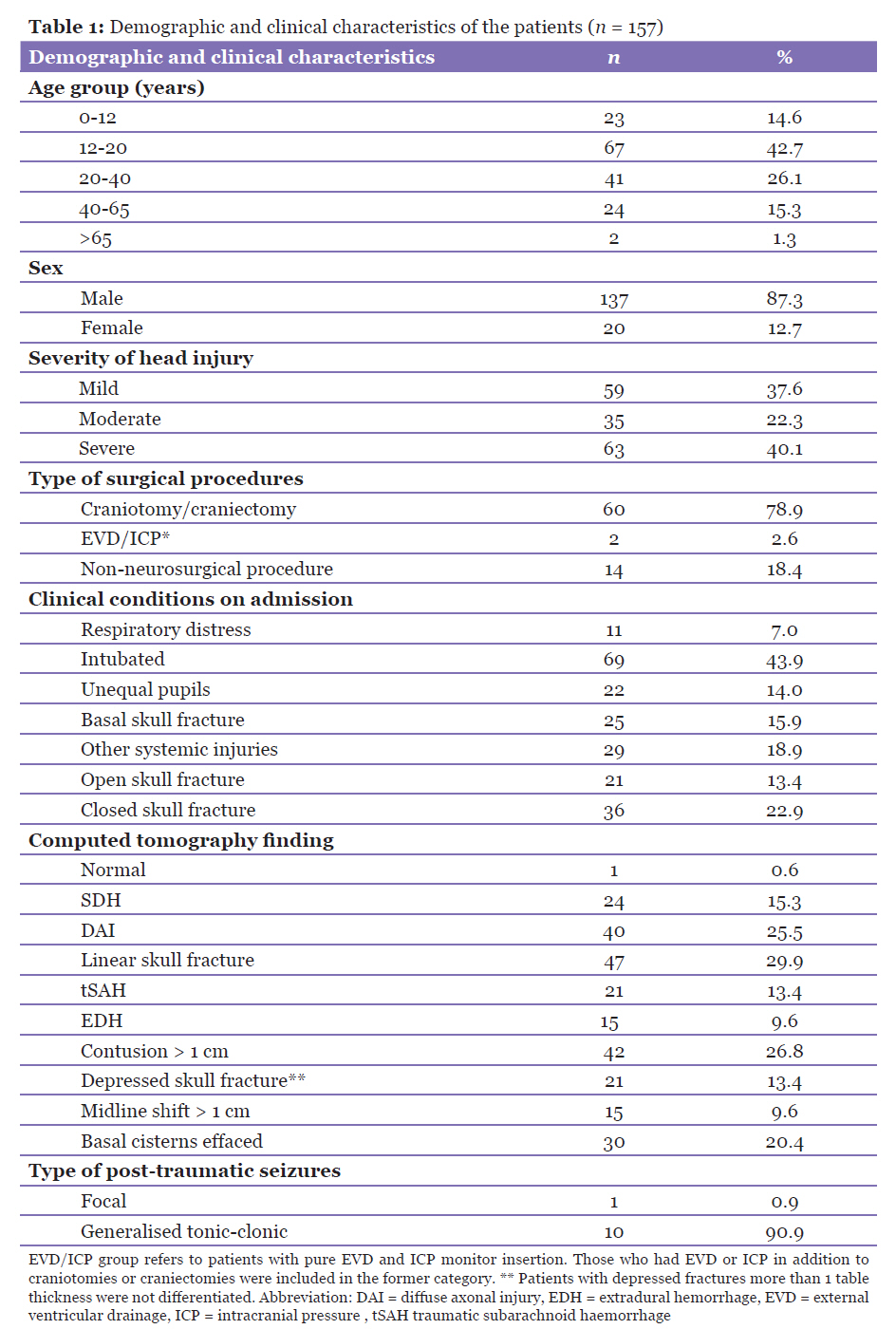
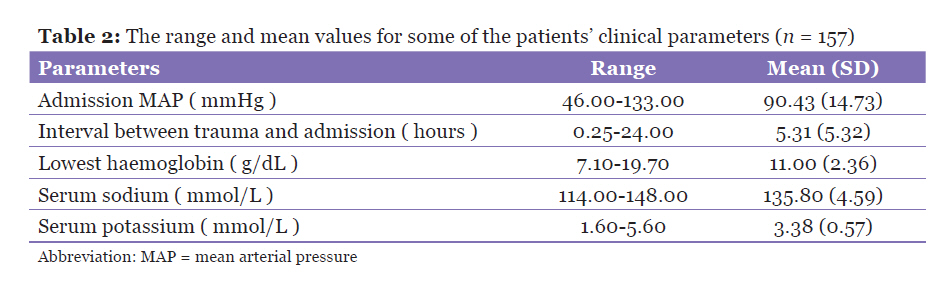
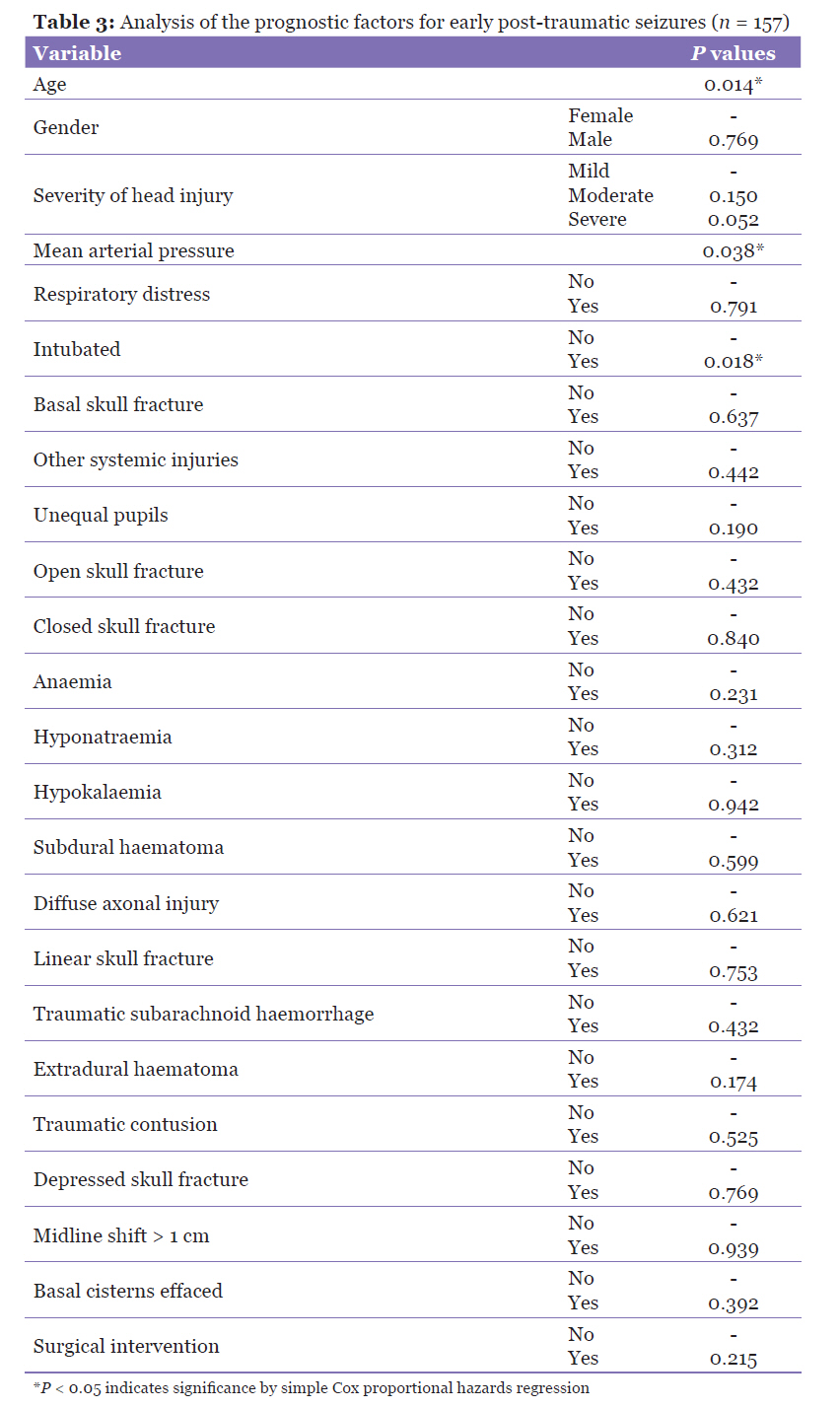
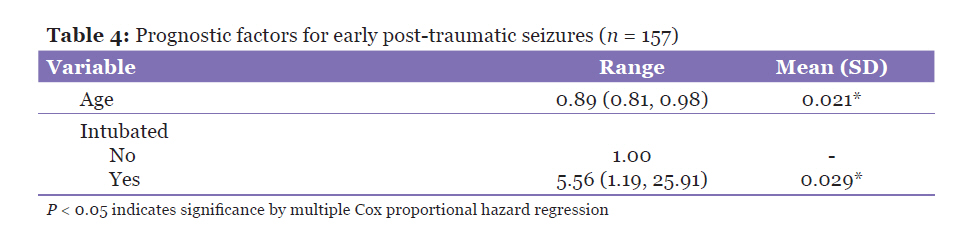
TBI was defined as an injury from external causes resulting in either a transient or a prolonged reduced level of consciousness, post-traumatic amnesia, or abnormal findings on computed tomography (CT) of the head. All of the patients who were included in the study were initially treated with the standard treatment protocols for managing head injuries as practised in HUSM. The relevant clinical data for the patients on admission and their subsequent progress were recorded. The CT scan findings were taken as those that were reported by the admitting neurosurgical resident and confirmed by senior lecturers. The site or multiplicity of intracranial haematomas or contusions were not differentiated. A baseline electroencephalogram (EEG) was scheduled for each patient during the course of the admission. The occurrence of any surgical procedure was also recorded. Surgical procedures were subdivided into craniotomy and craniectomy, insertion of ICP monitoring device or extraventricular drainage (EVD) catheter, and other non-neurosurgical procedures. For those who had more than 1 procedure, the more major procedure was recorded; for example, if a patient had both decompressive craniectomy and ICP monitor insertion, it was recorded under decompressive craniectomy. Patients were monitored continuously during admission for any seizure activity, and, on discharge, the patients and their caregivers were given information about the signs and symptoms of seizure activity. They were also given follow-up appointments every 3 months at the Neurosurgical Outpatient Clinic, HUSM, up to at least 1 year. Contact numbers were also obtained, and those who failed to attend an appointment were contacted by telephone to ascertain presence or absence of seizure activity. Data analysis was completed using SPSS version 12.1 (SPSS Inc., Chicago, IL). The significance level was set at P < 0.05. For the analysis of the risk factors, Cox proportional hazards regression was used to obtain the hazards ratio. This model was used because of the multiple covariates that were involved in the analysis. Simple Cox regression analysis was first used to determine which variables were significant, and these variables were then included in the multivariate analysis. The variables analysed were as follows: age; gender; severity of head injury on admission; clinical conditions on admission, such as respiratory distress, intubation, unequal pupils, basal skull fracture, other systemic injuries, as well as open or closed skull fractures; mean arterial pressure MAP on admission; haemoglobin, serum sodium and potassium levels; surgical intervention; phenytoin treatment; and CT scan findings, including diffuse axonal injury, traumatic subarachnoid haemorrhage, linear or depressed skull fracture, subdural haemorrhage (SDH), contusion, and extradural haemorrhage (EDH). Following the simple Cox proportional hazard regression analysis for single variables, the variables were selected for multiple regression analysis based on a P valueof less than 0.05. The covariates were then entered together, with the first category as baseline, a 95% confidence interval for the Hazard Ratio, and the Backward Likelihood (LR) test statistic as the automatic model selection method. Results A total of 157 patients were recruited in the study: 137 were male (87.3%), 20 were female (12.7%), and the male to female ratio was 6.85:1. The demographic and clinical characteristics of the patients are summarised in Table 1. The age of the patients ranged 2–87 years, with a mean (SD) age of 24.5(16.1) years. The majority of patients (42.7%) were in the 12–20 years age group. The most frequent admission Glasgow Coma Scale (GCS) was 7, in (17.8%) of patients. The patients were then divided into different categories of mild (GCS 13–15), moderate (GCS 9–12) and severe (GCS 3–8) head injury. The majority of the patients (n = 63, 40.1%) had severe head injury, while of those remaining, 59 (37.6%) had mild head injury and 35 (22.3%) had moderate head injury. The number of patients who underwent surgery was roughly the same as those who had non-surgical treatment, 81 (51.6 %) for no surgery versus 76 (48.4 %) for surgery. The patients who underwent surgical procedures were further categorised into types of surgical procedures. Of the 76 patients, 60 (78.9%) had either a craniotomy or craniectomy; 2 (2.6%) had EVD or ICP monitor insertion, while the remaining 14 (18.4%) had a non-neurosurgical procedure performed (such as plating of a fractured limb and maxillofacial procedures). Several other clinical conditions on admission were examined and recorded, namely presence of respiratory distress, status of intubation, unequal pupils, basal skull fractures, other systemic injuries, and open or closed skull fractures. CT scans of brain were done on all patients. The following characteristics were looked for: normal, subdural hemorrhage (SDH), diffuse axonal injury DAI, linear skull fracture, traumatic subarachnoid hemorrhage tSAH, extradural hemorrhage (EDH), contusion (more than 1 cm), depressed skull fracture, midline shift (more than 1 cm), and basal cisterns effaced. The range and mean values of the patients’ mean arterial pressure (MAP) on admission, interval between trauma and admission to HUSM, lowest haemoglobin (Hb), serum sodium, and serum potassium are summarised in Table 2. For the analysis of the prognostic factors, the variables analysed were age, gender, severity of head injury on admission, clinical condition(s) on admission (such as respiratory distress, intubation, unequal pupils, basal skull fracture, other systemic injuries, and open or closed skull fractures), MAP on admission, haemoglobin, serum sodium and potassium levels, surgical intervention, phenytoin treatment, and CT scan findings, (including diffuse axonal injury, traumatic subarachnoid haemorrhage, linear or depressed skull fracture, SDH, contusion, and EDH). The P values for all of these individual covariates as predictors of late post-traumatic seizures are summarised in Table 3. Following the simple Cox proportional hazard regression analysis for the single variables, 4 variables (age, severity of head injury, MAP on admission, and intubated on admission) were selected for the multiple regression analysis based on a P values of less than 0.05. Based on this final model, there were 2 significant risk factors in the development of early post-traumatic seizures: age (P = 0.021) and intubated patients (P = 0.029), as shown in Table 4. Discussion TBI is a major cause of morbidity and mortality worldwide, with an ever-rising trend. Severe head injury remains one of the leading causes of death and permanent disability in the young and productive age group in Malaysia, and causes a great burden and great economic loss to both the family and the country. The total number of road traffic accidents in Malaysia exceeded 223 000 in 1999 with an average of 16 deaths per day (8). In the Hospital Universiti Sains Malaysia, a total of 204 cases of head injury were admitted to the Neurosurgical Department in 2003, rising to 226 cases in 2004 and 231 cases in 2005. There were only 187 cases of head injury in 2006. However, the total rose to 189 cases in 2007 (9). Post-traumatic seizures can either be early, occurring within 1 week of the injury, or late, occurring from 1 week to years after the injury. Immediate seizures, occurring less than 24 hours after injury, is a third category (10,11). Recurring late seizures make up the clinical syndrome of post-traumatic epilepsy (2–4). Immediate and early post-traumatic seizures are important complications of head injury that need to be detected and treated, as seizure activity in this early period after a head injury can cause secondary brain damage due to increased metabolic demands, increased ICP, and excess neurotransmitter release (12). The incidence of early seizures ranges from 4%–25%, according to different references (3,5,13,14). In a study of 966 children, Ong et al. found the incidence of early post-traumatic seizures to be 5.5% (7). The 7.0% incidence of early post-traumatic seizures seen in this study is comparable with that from most series. While the study of Ong et al. focused mainly on the paediatric population (7), this study included all age groups, although its finding was that younger patients are more susceptible to early post-traumatic seizures. The risk factors for developing early post-traumatic seizures have also been studied in many case series. Early post-traumatic seizures could also be related to age, with Black et al. reporting a higher incidence in patients in the 2–14 years age group (3). Other risk factors reported include age greater than 65, chronic alcoholism, fractures at the base of the skull, and intracranial operations (13,15,16). In Ong et al.’s study, the significant risk factors were age less than 2 years, female sex, loss of consciousness for more than 24 hours, and acute subdural haematoma (7). The results from this study show that for early post-traumatic seizures, the risk factors are younger age and intubated patients. In our results, for every increase of 1 year in age, the hazard of developing an early post-traumatic seizure was 0.89. However, no age group or age limit was found for this risk. The other group of patients at higher risk for early post-traumatic seizures was those who were intubated at admission. The main indications for intubation were a GCS of 8 and below (48 of 69) and respiratory distress (10 of 69) and chest injury (1 of 69). This group of patients were found to be more severely injured (81.0% had a GCS score of 3–8). About half (53.4%) of the patients who were intubated also underwent surgery, with craniotomies and craniectomies being the most common operations (74.1%). This result could indicate that the severity of the head injury and open cranial surgery could be related to the development of early seizures. Furthermore, about 20.0% of these patients were intubated due to respiratory distress or severe chest injury. This may indicate that hypoxia could also play a role in the development of early post-traumatic seizures. However, as pre-intubation arterial blood gases were not available, this relationship could not be ascertained and could be included in future studies. Other conditions (such as subdural haematomas, contusions, skull fractures, or contusions) were not significant in this study. As mentioned earlier, treatment of early and late post-traumatic seizures can have an important bearing on outcome. Adequate control of early seizures can help prevent secondary brain damage, while control of recurring late seizures can improve a patient’s rehabilitation and reintegration into society. Numerous regimens and drugs have been studied and proposed in this respect, with some contrasting results. Temkin et al. found that phenytoin and carbamazepine are effective in preventing early seizures, but not effective in preventing late seizures (12). Pechadre et al. treated 34 out of 86 patients with severe head injuries with a loading dose of intravenous phenytoin followed by oral phenytoin administration for at least 3 months (17). After 2 years follow-up, there was a significant difference between the treated and untreated patients (17). Murri et al. found that phenobarbital at 1.5 mg/kg/day had an efficient prophylactic effect against late post-traumatic seizures (18). Schierhout and Roberts did a systematic review of randomised controlled trials on post-traumatic seizure prophylaxis and concluded that prophylactic antiepileptic drugs are effective in reducing early seizures, but have no benefit against late seizures or death and neurological disability (19). In 2003, the American Academy of Neurology issued a practice parameter for the use of antiepileptic drug prophylaxis in severe TBI. The conclusions were that in adult patients with severe head injury, phenytoin prophylaxis is effective in decreasing the risk of early post-traumatic seizures. However, antiepileptic drug prophylaxis is probably not effective in decreasing late post-traumatic seizures (20). The results of this study are comparable to the above-mentioned recommendations, in that phenytoin was not found to be an effective as a prophylaxis against late post-traumatic seizures. Conclusion This study showed that the incidence of early post-traumatic seizures in the local population of Kelantan and Terengganu was 7.0%, which is comparable to incidence rates elsewhere. Younger and intubated patients were at a higher risk of developing early post-traumatic seizures. Because any seizure event could have an adverse effect on morbidity and mortality, it may be necessary to give antiepileptic prophylaxis in this group of patients. This study, even though in a small cohort, suggests that administration of antiepileptic drug was not beneficial in preventing late post-traumatic seizures but may have a role in preventing early seizures. Future studies on a larger number of patients with a longer follow-up period may be able to answer these doubts. Acknowledgements We would like to thank the Director of HUSM, Dr Zaidun Kamari, for the hospital’s support and all HUSM neurointensive care nurses who helped to complete the study. Authors’ Contributions Conception and design: CKH, JT References
© Copyright 2010 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj10046t2.jpg] [mj10046t1.jpg] [mj10046t4.jpg] [mj10046t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}