 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
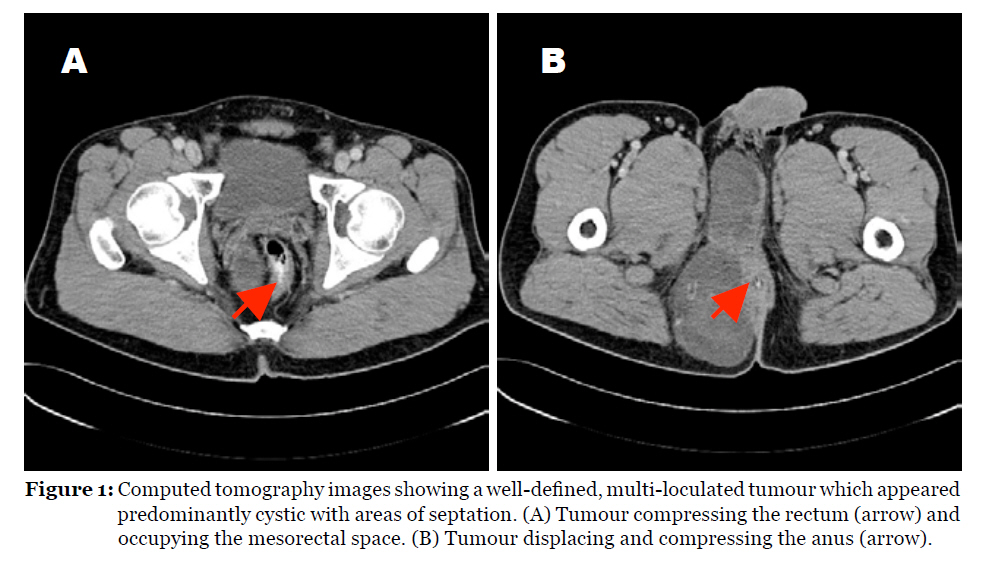
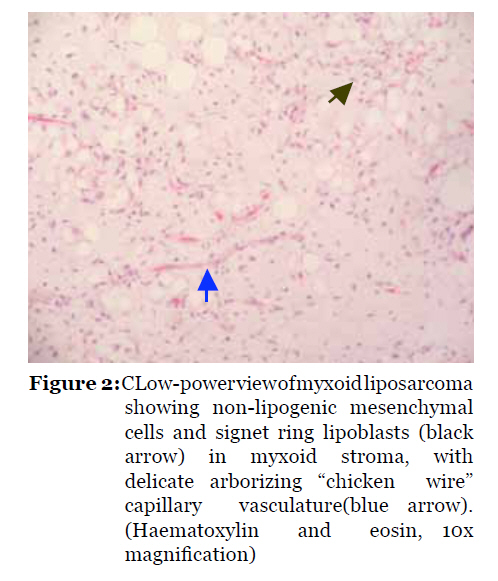
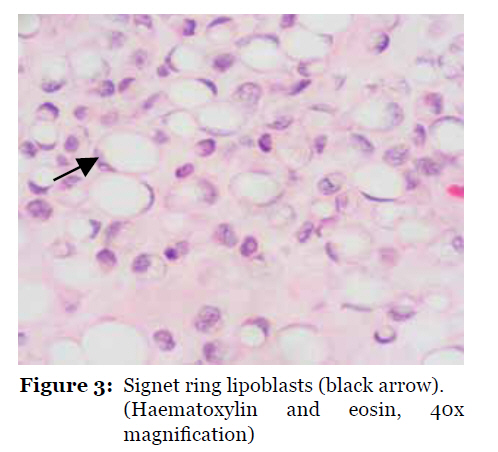
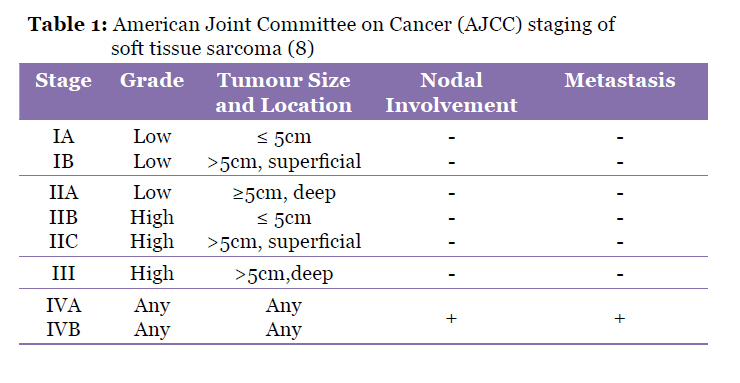
Malaysian Journal of Medical Sciences, Vol. 17, No. 3, 2010, pp. 62-66 Case Report Perineal Myxoid Liposarcomas: A Case Report and Literature Review Prabhu Ramasamy1, Azmi Md Nor1, Nil Amri M Kamil1, Norra Harun2, Mubarak M Yusof3, Mohd Zailani Md Hassan1 1Colorectal Unit, Department of Surgery, Faculty of Medicine, International Islamic University Malaysia, 25100 Kuantan, Pahang, Malaysia Correspondence: Professor Dr Azmi Md Nor, MD(USM), MS(UKM), Colorectal Unit, Department of Surgery, Faculty of Medicine, International Islamic University Malaysia, 25100 Kuantan, Pahang, Malaysia, Tel: +609-5146090 Fax: +609-5146090 Email: azmimn@iiu.edu.com Submitted: 30 Dec 2009 Code Number: mj10050 Abstract Myxoid liposarcoma is the major subtype of liposarcoma and commonly presents in the extremities, particularly in the thigh. We introduce an unusual case of a myxoid liposarcoma presenting as a large perineal swelling occupying the para-rectal and para-anal spaces in a 49-year-old male patient. The diagnosis, management, and prognosis of myxoid liposarcoma are discussed. A literature review is performed for myxoid liposarcoma. Keywords: myxoid liposarcoma, oncology, perineum, soft tissue sarcoma, surgery, tomography Introduction Liposarcomas are rare soft tissue tumours, with an incidence of 30 cases per 1 million individuals. Myxoid liposarcoma (MLS) is a major subtype of these liposarcomas (1). It represents approximately 30%–50% of all the liposarcomas. Most patients present between the ages of 18 and 67 years, with a mean age of 42 years (2–4). MLS has the potential for overt malignant behaviour, and therefore determination of clinical behaviour and pathological subtype is invaluable to the management of these patients. We report a rare presentation of perineal MLS. The diagnosis, management, and prognosis will be discussed. Case Report A 49-year-old Malay man presented with a swelling in the right perineal region of 1 year’s duration. When initially noticed, the swelling was thumb-sized but had increased gradually over the next few months to the size of a fist. The swelling was associated with a mild, dull aching pain. He gave no history of bowel or other constitutional symptoms. Clinical examination revealed a swelling extending from the right perineum laterally to the right gluteal region, with extension anteriorly to the base of the penis and posteriorly to the tip of the coccyx. It measured approximately 16 x 10 cm. The clinical impression was that the tumour was in the subcutaneous plane and had the consistency of a lipoma. Digital rectal examination revealed the presence of an extra luminal compression over the right and posterior aspect of the lower rectum. The patient was claustrophobic and therefore refused a magnetic resonance imaging (MRI) examination. A computed tomography (CT) scanning of the abdomen and pelvis was performed. It revealed a well-defined, multi-loculated mass arising posterior to the right seminal vesicle. The mass extended inferiorly into the mesorectum and right ischioanal space. It compressed and displaced the rectum to its left. The mass extended towards the symphysis pubis inferior to the shaft of the penis. The maximum cranio-caudal width and anterior–posterior dimensions were 16 x 8 x 14 cm. The mass appeared predominantly cystic with areas of septation (Figure 1). Based on these findings, the differential diagnosis of lymphangioma or a tailgut cyst was considered. In view of the radiological diagnosis, a biopsy was not taken. After consultation with the patient, a decision was made to operate. Wide excision of the tumour was performed via a perineal approach by the colorectal surgeon. Intra-operative findings revealed a well-encapsulated, multi-loculated tumour with areas of admixed fatty, cystic, and solid components. The histological examination revealed round to oval mesenchymal cells and signet ring lipoblasts in a myxoid stroma (Figure 2). The cells had hyperchromatic nuclei with conspicuous nucleoli and scanty cytoplasm (Figure 3). The stroma was rich in delicate, arborizing capillary vasculature, which is also described as a “chicken wire” appearance (Figure 2). The tumour, with predominantly myxoid matrix and lipoblasts, conformed to the diagnosis of MLS. The round cell component comprised 10% of the cell field. The resected margins were close. The patient was subsequently referred to the oncologist for adjuvant therapy. He was given radiotherapy consisting of a total of 65 Gy over 45 fractions to the tumour bed and 10 Gy to the operative scar. The patient was followed up every 6 weeks for the first 6 months and every 3 months thereafter. On his first 6-month follow up after surgery, clinical examination and CT scan showed no local recurrence or distant metastasis. Discussion Liposarcoma is the second most common soft tissue tumour, and MLS is a major subtype, consisting of 30%–55% of these tumours (2,3). MLS commonly involves the thigh and retroperitoneum, but it is relatively rare in the perineum or pararectal spaces (1,2). Clinically, these tumours present as painless swellings that progressively increase in size. They usually grow to a considerable size before they become symptomatic. In the case of our patient, he remained asymptomatic even though the tumour occupied his right pararectal and perianal spaces with the displacement of the anus. A multi-imaging technique approach is often necessary for an accurate pre-operative evaluation, diagnosis, and staging of MLS. This approach helps to ensure curative resection with adequate surgical margins, thereby minimizing the risk of local recurrence. MLS presents a unique radiological challenge. The tumours exhibit a spectrum of MRI signal intensities and CT attenuation. A major contributing factor is the low fat content (less than 10%–25% of the tumour volume), while other contributors are the quantity of mucinous and myxoid materials, vascularity, and necrosis within the tumour (4). These tumour characteristics explain why the signal is close to that of water on non-enhanced CT and MRI scans (4). As encountered with this patient, the administration of contrast produced little enhancement on CT. Hence, the images mimic those of a cyst (2,4). Gadolinium-enhanced MRI is the imaging of choice for MLS, where cystic or necrotic lesions are distinguishable from solid or cellular lesions (1,2). Sung et al. reported that 96% of MLS appeared as solid masses with varying patterns of enhancement using gadolinium-enhanced MRI (4). On MRI, the enhancement patterns are classified into homogeneous, heterogeneous, and no enhancement (4). Unfortunately, due to the patient’s claustrophobia, the MRI scan was not performed. In his case, the use of ultrasonography, especially endoanal ultrasonography, might have been useful to differentiate the solid from cystic components (2). Despite the shortcomings in imaging this patient, adequate pre-operative assessment of the tumour extent was obtained. This assessment allowed the planning and positioning of the incision and resection of the tumour with the preservation of the pelvic organs and continence Surgery remains the mainstay of treatment for MLS (1,2). An adequate margin is required to prevent local recurrence, as it is associated with a 2.8-fold risk of disease mortality (5). A wide surgical margin should always be attempted, unless there are vital structures in proximity; in these circumstances, post-operative radiotherapy is recommended for adequate local disease control (1,5). In the present case, the tumour proximity to the anus prevented a wide surgical margin. The classical histological appearance of MLS is characterized by the presence of myxoid matrix with a signet-ring type lipoblast and a capillary network that creates the appearance of “chicken wire” (7). When MLS is associated with a round cell component that exceeds 5% of the tumour, it is considered a round cell liposarcoma, RCLS (5). Currently, the pure MLS and RCLS are generally considered to be of the same subtype; pure MLS is described as being of low grade with low metastatic potential, whereas the RCLS represents the opposite end of the spectrum (5,7). The demonstration of chromosome translocation t(12;16)(ql3;pl1) in both MLS and RCLS serves as genetic evidence for the hypothesis that they are of the same subtype (5). There is no specific grading or staging system for liposarcomas; they are broadly graded and staged as soft tissue sarcomas. Among the various scoring systems available are the American Joint Committee on Cancer (AJCC) and Enneking staging systems (6,9). The AJCC system (Table 1) is commonly used on account of its reproducibility and reliability (8). The factors considered in the grading of these tumours in the AJCC system are cytological atypia (differentiation), tumour necrosis, and mitotic counts. In this system, the grading is considered low (I, II) or high (III, IV) only (8). This reduces intra- and inter-observer variations of grading and its effects on the tumour staging. The rates of local recurrence for MLS are relatively high at about 40%–50% of the cases. Pure MLS has a 20% rate of metastasis, which compares to its round cell subtype that metastasizes in almost 35%–70% of the cases. Common metastatic sites include lungs, bones, and occasionally, the serosal surfaces of the pleura, pericardium, and peritoneum (1,2). The 5 and 10 year survival rates are 80% and 50%, respectively (3,5). A major predicting factor for local recurrence is the surgical margins; for metastasis, the factors are the histological grade and the percentage of round cells (1,5). There is no consensus on the use of neo-adjuvant and adjuvant therapies in the form of chemotherapy or radiotherapy for non-metastatic soft tissue sarcomas (9). Surgery is therefore followed by an adjuvant radiation therapy only if the resection margins are deemed inadequate, as was the case in this patient. Chemotherapy with doxorubicin and ifosfamide is usually reserved for treatment of metastatic disease (7,10),. The use of chemotherapy for high-grade tumours and local recurrence is controversial (9). MLS is relatively more chemo-sensitive when compared to other soft tissue sarcomas as a group (7). After the completion of treatment, a scheduled follow-up should be commenced in the form of clinical examinations and imaging (preferably MRI) performed every 6 months for 5 years and then annually for at least 5 years after (1). Conclusion MLSs are rare soft tissue sarcomas that have benign clinical presentation. Pre-operative radiological diagnosis is crucial for staging and surgical planning. Surgery remains the mainstay of treatment for both non-metastatic and metastatic disease. The quality of the surgical margins greatly affects the patient’s prognosis. Proper histological typing and grading will help determine the metastatic potential of this sarcoma. These factors will further aid in detection of local recurrence and distant metastasis. Acknowledgement We wish to thank Professor Amjad for reviewing the manuscript and all the staff of Department of Surgery, Hospital Tengku Ampuan Afzan and International Islamic University Malaysia for their support. Authors’ Contributions Conception and design: AMN, MZMH References
© Copyright 2010 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj10050f1.jpg] [mj10050t1.jpg] [mj10050f2.jpg] [mj10050f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}