 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 18, No. 1, 2011, pp. 38-44 Original Article Peripheral Blood Lymphocyte Subset Counts in Pre-menopausal Women with Iron-Deficiency Anaemia Mohammad Reza KERAMATI 1, Mohammad Hadi SADEGHIAN2, Hossein AYATOLLAHI2, Mahmoud MAHMOUDI3, Mohammad KHAJEDALUEA4, Houman TAVASOLIAN5, Anahita BORZOUEI5 1Neonatal Research Center, Imam Reza Hospital, Faculty of Medicine,
Mashhad University of Medical Sciences, Mashhad, Iran Correspondence: Dr Mohammad Hadi Sadeghian,
MD (Mashhad University of Medical Sciences),
Hematology and Blood Banking Department,
Ghaem Hospital, Mashhad University of Medical Sciences,
Mashhad, Iran,
Tel: + 985518012363 Submitted: 11 May 2010 Code Number: mj11007 Abstracts Background: Iron-deficiency anaemia (IDA) is a major worldwide public health
problem. Children and women of reproductive age are especially vulnerable to
IDA, and it has been reported that these patients are more prone to infection.
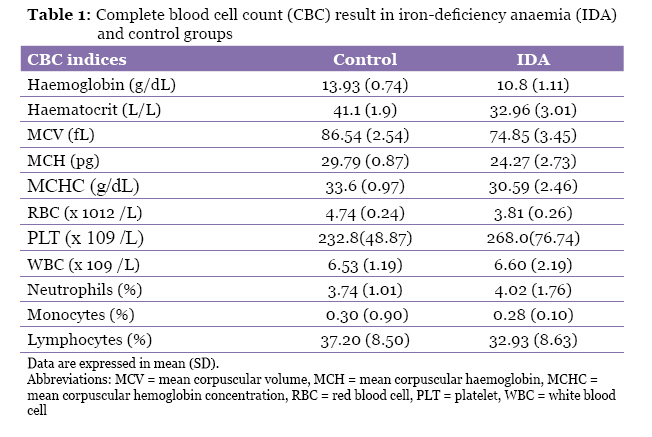
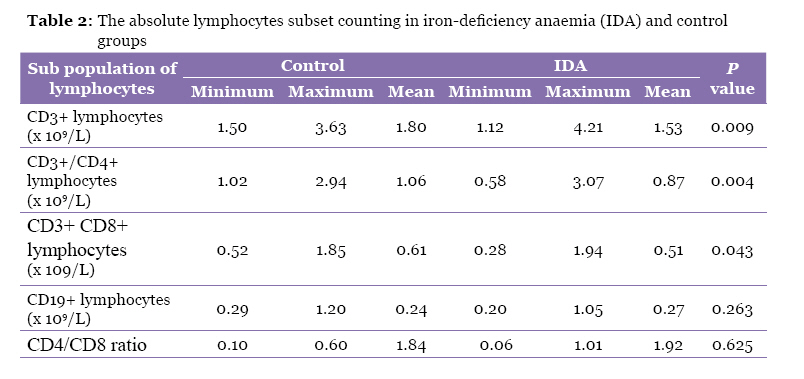
This study was done to evaluate alteration of lymphocyte subgroups in IDA. Keywords: flow cytometry, immunology, iron-deficiency anaemia, pre-menopause, T lymphocytes, women Introduction Iron deficiency is one of the most common known forms of nutritional deficiency in the world. Iron-deficiency anaemia (IDA), which occurs due to nutritional deficiency, is a major health problem in developed and developing countries. IDA is characterised by a defect in haemoglobin synthesis, resulting in red blood cells that are abnormally small (microcytic) and contain a decreased amount of haemoglobin (hypochromic). The prevalence of IDA varies according to sex, age, and geography. Young children and menstruating women are at higher risk for IDA because of higher iron needs (1). The prevalence of IDA has been reported to be 40% of adult males and 57% of adult females in South Asia, 2%–5% of adolescent girls and women of childbearing age in the US, 19% in France, 20% in Poland, 36% in Lebanon, 28% in India, and 21% in Turkey (2–9). Although the overall frequency of IDA in Iran is not well documented, it appears to be common based on some reports. For example, in one study performed in north Iran, the prevalence of anaemia based on serum iron index and haemoglobin was 24.2% and 18.2%, respectively, in pregnant women and 21.2% and 21.0%, respectively, in non-pregnant women (10). Altered immune responses have considerable public health significance. The relationship between iron deficiency and infection susceptibility has been investigated. There is some evidence that iron is a fundamental element for normal development of the immune system and some clinical studies have emphasised the importance of iron in the integrity of the immune system (11–14). Tang et al. observed that the incidence of infectious diseases in IDA patients was significantly higher than that in the control group (15). Furthermore, it has been suggested that iron supplementation can improve iron levels and reduce morbidity from upper respiratory tract infections in children with or without infection (16). Tang et al. (15) and Feng et al. (17) reported lower levels of immunoglobulin (Ig) G in children and pregnant women with IDA. A correlation between iron intake and IgG levels in athletes has also been reported by Kim et al. (18). Changes in serum complement levels were also observed in anaemic patients (17). The effects of iron deficiency on cellular immune function remain controversial. Some reports indicate that iron depletion may be responsible for decreased cellular immunity while others have not reported any changes in lymphocyte subset in patients with IDA (19,20). Most studies include data obtained from anaemic children and few reports exist concerning adults with IDA. It is important to understand the effects of IDA on the immune system due to its high prevalence. Lymphocyte subsets in 50 pre-menopausal adult females with IDA were studied and the results were compared with those of a control group. The aim of this study was to show whether peripheral blood lymphocyte subsets change in adult non-pregnant females with IDA. Subjects and Methods This prospective study was conducted on non-pregnant, pre-menopausal female patients referred to the Hematology and Blood Banking Department of Ghaem Hospital, Mashhad University of Medical Sciences (MUMS), Mashhad, Iran, from April 2008 to January 2009. The voluntary subjects were included in this study, and each patient’s medical history was obtained and recent laboratory results reviewed. A total of 50 non-pregnant, pre-menopausal women between the ages of 20–45 years old presenting with IDA as the solitary pathology were included in the patient group. The inclusion criteria were haemoglobin (HGB) level of less than 12.5 g/dL, red blood cell (RBC) count of less than 4 x 1012/L, mean corpuscular volume (MCV) of less than 80 fL, mean corpuscular haemoglobin (MCH) of less than 27 pg, serum iron level of less than 50 µg/dL, total iron binding capacity (TIBC) of more than 400 µg/dL, and serum ferritin level of less than 20 µg/dL. The exclusion criteria were possible thalassaemia according to the laboratory results, a history of acute or chronic infection, familial history of immunodeficiency, history of cancer, pregnancy, and a history of endocrinopathy, especially hypo- or hyperthyroidism. Fifty healthy, asymptomatic women were selected as the control group during the same period based on recent routine laboratory results. Inclusion criteria were absence of anaemia and iron deficiency with HGB level of 13–16 g/dL, RBC count of 4–6 x 1012/L, MCV of 80–96 fL, MCH of 27–33 pg, serum iron level of 50–150 µg/dL, TIBC of 250–400 µg/dL, and serum ferritin level of 20–200 µg/dL. Patients in the control group had no history of chronic disease or drug consumption during the previous 6 months. The iron-deficient and control groups were comparable with respect to the sex and age. Four millimetres of the venous blood of controls and patients were collected in 2 sterile tubes containing K3–EDTA anticoagulant for complete blood cell count (CBC) and flow cytometry analysis. CBCs were obtained using a calibrated electronic counter, Sysmex Kx-21 (Sysmex Corporation, Kobe, Japan). Peripheral blood smears (PBS) were prepared with Geimsa staining and white blood cell (WBC) differential counting in PBS was completed to control for the absolute lymphocytes counts and percentage of lymphocytes reported by cell counters. One tube from each subject was sent to Bouali Research Center laboratories of MUMS for flow cytometric analysis of peripheral blood by a fluorescence-activated cell sorting (FACS) count flow cytometer (Becton, Dickinson, and Company, San Jose, CA, USA) using monoclonal antibodies (Becton, Dickinson, and Company, San Jose, CA, USA) specific for CD3, CD19, CD45, CD4, and CD8 lymphocyte antigens for determining the percentage of these lymphocyte subpopulations in the samples. All samples were taken at the same time of day (usually at around 8:30 am). Specimens were kept at room temperature, transported to the Bouali Research Center laboratories of MUMS, and analysed by flow cytometry as soon as possible (usually within 2 hours). In flow cytometry histograms, lymphocyte gating was set using linear 90° side-scatter and log CD45 fluorescence. Lymphocytes are CD45-positive cells with low side scatter. T (thymus-derived) and B (bone marrow-derived) lymphocytes were separated by CD3 and CD19 markers in the lymphocyte regions of flow cytometer histograms, then the expression of CD4 and CD8 markers were evaluated in the CD3-positive cell population. CD3 positive CD4 positive (CD3+/CD4+) and CD3 positive CD8 positive (CD3+/CD8+) cells were considered as T helper and T cytotoxic lymphocytes, respectively. The absolute lymphocyte subsets were calculated by multiplying the percentage of these lymphocyte subpopulations (results of flow cytometry) by absolute lymphocyte counts (results of CBC). Quantitative variables were expressed as mean (SD). The percentage of lymphocyte subsets and absolute lymphocyte subset counts in two groups of IDA patients and controls were analysed with SPSS Version 11.5 (SPSS Inc., Chicago, IL, USA) by a statistician using one-sample Kolmogorov–Smirnov test for evaluation normality of the data distribution and then using t test to compare mean values between case and control groups. A P value of less than 0.05 was considered statistically significant. Results The age range in the control group was from 20 to 45 years (33.3 ± 9.76 years) and in IDA group (case group) was from 20 to 45 years (31.7 ± 7.01 years), and t test analysis showed no significant differences between case and control groups (P = 0.34). The mean haemoglobin, haematocrit, red cell indices, and RBC counts were significantly lower in the iron-deficient group. In contrast, the PLT (platelet) count in IDA group was higher than that of the control group (Table 1). Statistical analysis by t test showed significant differences between these two groups for all red blood cell indexes (P < 0.001). The PLT count was significantly higher (P = 0.008) and the percentage of lymphocytes was lower (P = 0.014) in the IDA group as compared with the control group. There were no statistically significant difference between the two groups for mean relative counts of WBC (P =0.83), or percentage of neutrophils (P =0.10) and monocytes (P =0.14). The mean percentages of lymphocyte subsets were 75.38%, 58.58%, 34.04%, and 10.20% for total T lymphocytes (CD3+), T helper (CD3+/CD4+), T cytotoxic (CD3+/CD8+), and B cells (CD19+), respectively, in the control group, and 73.20%, 58.06%, 33.10%, and 13.06% in the IDA group. Although the mean percentages of CD3+, CD3+/CD4+, and CD3+/CD8+ lymphocytes in the iron-deficient group were lower compared with those in the controls, these differences were not statistically significant with P values of 0.20, 0.75, and 0.53, respectively. The absolute lymphocyte subset counts in the iron-deficient and control groups are shown in Table 2. The mean (SD) absolute CD3+, CD3+/CD4+, CD3+/CD8+, and CD19+ lymphocyte counts were 1.80 (0.48), 1.06 (0.34), 0.61 (0.19), and 0.24 (0.11) x 109/L, respectively, in control subjects, and 1.53 (0.53), 0.87 (0.28), 0.51 (0.24), and 0.27 (0.15) x 109/L, respectively, for the IDA group. The absolute T lymphocytes (CD3+) and subpopulations (CD4+, CD8+) in the iron-deficient group were significantly lower than in the control group. Statistically significant differences in CD4:CD8 ratios and numbers of CD19+ lymphocytes between the two groups were not seen. A Pearson correlation test showed a significant correlation between the absolute T and B lymphocyte populations (r = 0.565, P < 0.001) and between the absolute CD4 and CD8 lymphocytes (r = 0.357, P < 0.001). Discussion Iron deficiency is one of the most common preventable nutritional deficiencies in developed and developing countries. IDA can cause irritability, headache, and fatigue that change social behaviour and impair the ability of adults to do physical work (1,3,21). An increased susceptibility to infections has been reported in some IDA patients, the aetiology of which is not well-known (11–15). Iron is crucial for cell proliferation due to its role in DNA synthesis and maturation of T lymphocytes. It is essential for enzymes such as ribonucleotide reductase, and it is involved in DNA synthesis; therefore, the proliferative phase of lymphocyte activation is an iron-requiring step and this activity can be diminished during IDA (22). Some authors have suggested that altered levels of some interleukins (IL) and cytokines (e.g. IL-2, IL-1, IL-6, TNF-α, IL-4, IL-12p40, IFN-γ, and IL-10) might lead to immune system impairment in IDA patients (23–25). In addition, it has been suggested that altered cell marker expression may contribute to reduced T cell proliferation during iron deficiency (26). Cellular immunity and humoral immunity is mediated by T and B lymphocytes, respectively. T lymphocytes proliferate in the thymus and released into the peripheral blood where they constitute 60% to 70% of total blood lymphocytes. Cellular immunity protects the body by the production of cytotoxic T lymphocytes, activated macrophages, and activated NK cells, and it is mediated mainly by T lymphocytes. Cell-mediated immunity is responsible for defence against intracellular microbes (27). Mature T cells are of at least three types. The T helper cells express CD3+/CD4+ cell markers, while T suppressor/cytotoxic cells express CD3+/CD8+ cell markers. Mature T cells with γ/δ T cell receptor chains exhibit CD2+, CD3+, and CD7+, and lack CD4 and CD8; these type of T cells seem to function as another population of cytotoxic cells. Our findings showed significant decreases in total CD3+, CD3+/CD4+, CD3+/CD8+, and T lymphocyte counts in IDA patients. These were consistent with some earlier studies (29–32). Lower levels of mature T lymphocytes (CD4+ and CD8+) were observed in 40 IDA children by Attia et al. (30). A relationship between iron deficiency and cell-mediated immunity in children was also studied by Mullick et al.; the research was done on 40 iron-deficient and 30 healthy children and the authors also reported significantly decreased mature T lymphocytes (CD3+), helper–inducer T lymphocytes (CD4+), and CD4:CD8 ratios in iron-deficient versus iron-sufficient children. Although slightly lower means of CD8+ lymphocyte counts were observed by Mullick et al. (31), these differences were not significant. In contrast to our results, no difference in the distribution of T lymphocyte subgroups was found by Ekiz et al. and Thibault et al. (33,34). The previous discrepancies may be due to different sample size, age, sex, nutritional status, and host immune responses. The majority of similar previous studies were completed with paediatric patients (29–34). We selected non-pregnant menstruating women who were prone to IDA. Furthermore, the sample size in our study was slightly greater than that reported in previous studies. Mullick et al. (31) and Attia et al. (30) reported that iron supplementation improved T lymphocyte counts. This improvement was not observed by Tsouchnikas et al. (35) or Sejas et al. (36). The difference between the mean CD4:CD8 ratio in the iron-deficient group and control group in our study was not found to be statistically significant. Reports by other authors regarding the CD4:CD8 ratios in IDA are variable. Luraschi et al. (37) showed decreases in CD3+ and CD8+ levels and increases in the CD4+/CD8+ cell ratio. In contrast to our study, lowered levels of CD3, CD4, and CD4/CD8 ratios were reported by Mullick et al. (31). Our observations that the iron-deficient women had significantly lower mean levels of CD3+ lymphocytes in comparison with the control group were consistent with these reports. We found that there was no significant difference for the absolute number of B lymphocytes (CD19+ cells) in IDA patients versus the control group. This finding was concordant with some earlier studies (38). In our study, an increase in platelet counts in IDA patients compared with the control group was seen and this increase was statistically meaningful and consistent with some other reports (39,40), although other studies were not in agreement with ours (41,42). Leukocyte counts in the two groups were not statistically different, where this was again consistent with some previous studies (1,27). Conclusion We found significant changes in the total lymphocyte counts, T lymphocyte numbers, and distribution of T cell subgroups (lower CD3+/CD4+ and CD3+/CD8+ T lymphocytes count) in women with IDA. This study showed that absolute counts of peripheral blood T lymphocytes, as a marker of cell-mediated immunity, may be decreased in pre-menopausal women with IDA and that these patients may be more prone to infection. Acknowledgements This study was financially supported by the Research Council of Mashhad University of Medical Sciences. The authors are thankful to the Council and Miss Hoda Enaiati, Miss Masoumeh Mahmoudi, and Miss Nafise Tabasi for their kind assistance in conducting the laboratory tests. Authors’ Contributions Conception and design: MRK References
© Copyright 2011 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj11007t2.jpg] [mj11007t1.jpg] |
| |||||||||

{kind=link}
{kind=link}