 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
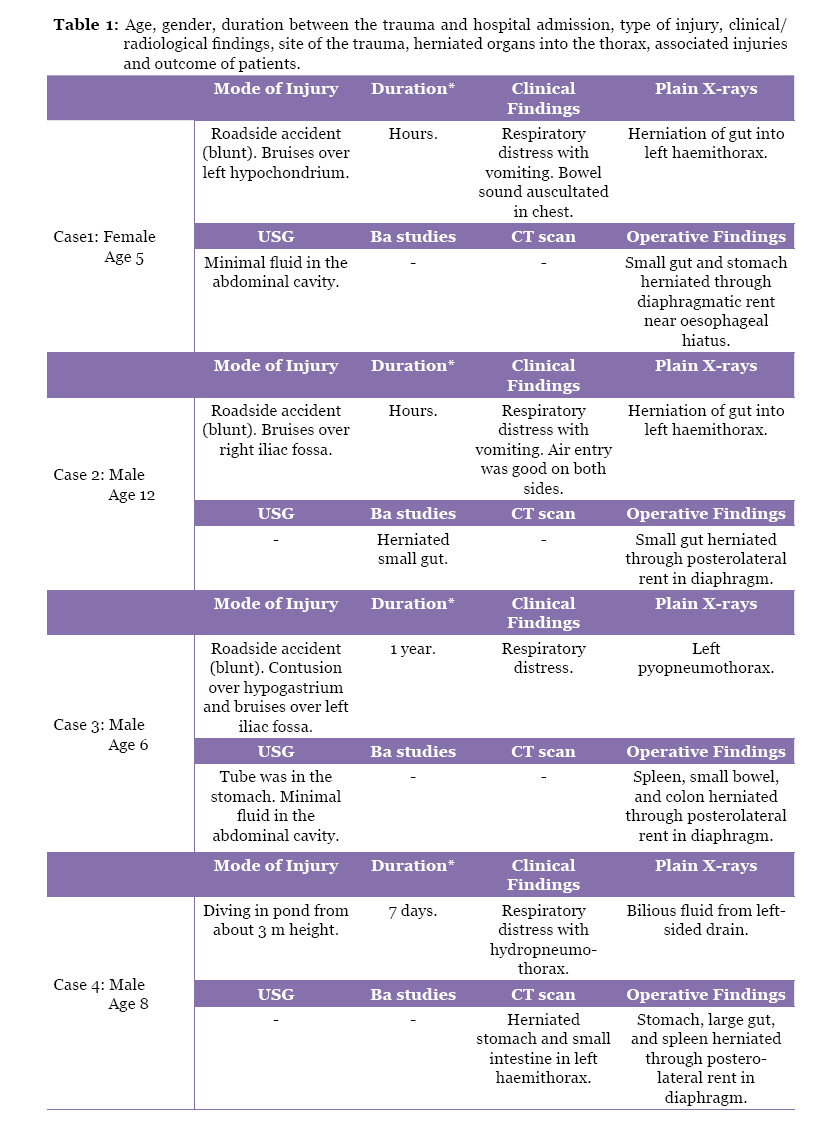
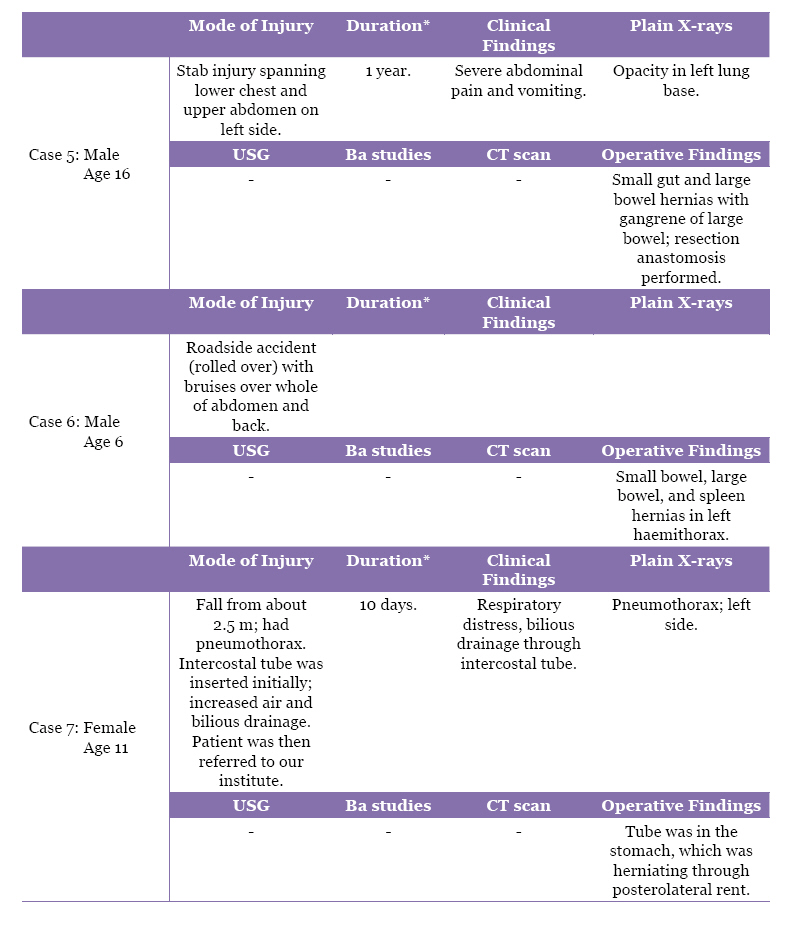
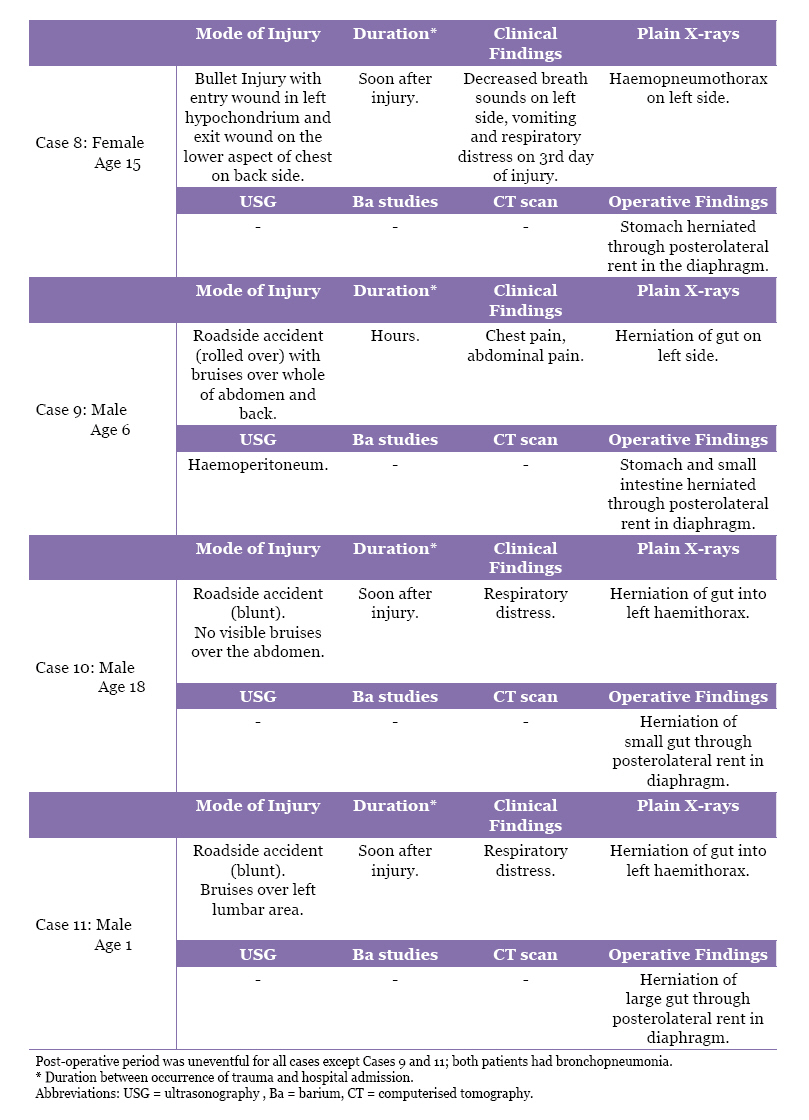
Malaysian Journal of Medical Sciences, Vol. 18, No. 1, 2011, pp. 45-51 Original Article Thirteen Years’ Experience of Diaphragmatic Injury in Children from the Post Graduate Institute of Medical Sciences (PGIMS), Rohtak, India Kamal Nain RATTAN1, Rajat NARANG1, Seema ROHILLA2, Sarita MAGGU2, Dhara B DHAULAKHANDI3 1Department of Pediatric Surgery, Post Graduate Institute of Medical Sciences,
Pt BD Sharma University of Health Sciences, Rohtak 124 001, Haryana, India Correspondence: Dhara B Dhaulakhandi, PhD Cell and Molecular Biology, Otolaryngology (All India Institute of Medical Sciences), Department of Biotechnology & Molecular Medicine, Post Graduate Institute of Medical Sciences, Pt BD Sharma University of Health Sciences, Rohtak 124 001, Haryana, India, Tel: +91-9416312237 Fax: +91-1262-211911 Email: BTMM.submissions@gmail.com Submitted: 6 Apr 2008 Code Number: mj11008 Abstract Background: Diaphragmatic hernia is migration of abdominal viscera into the
thoracic cavity through a defect in the diaphragm. In children, it is mostly
congenital; traumatic diaphragmatic hernia being less common. This study aimed
to review our experience with traumatic diaphragmatic rupture (TDR) and to
identify the clinical findings and diagnostic modality that may help in early
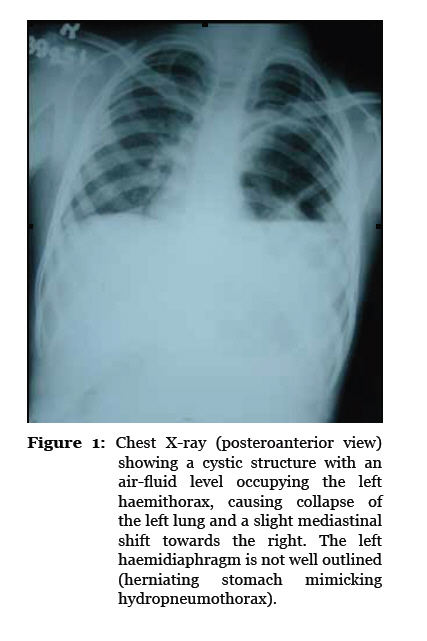
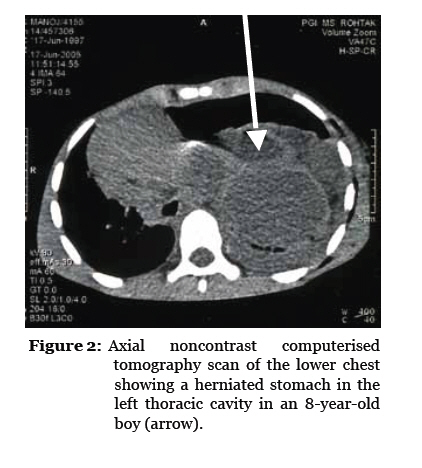
diagnosis and prompt therapy. Keywords: acute respiratory distress syndrome, child, diagnosis, diaphragmatic hernia, medical imaging, rupture, trauma Introduction Diaphragmatic rupture is an uncommon but well-recognised complication of trauma that consists of 1.0%–5.8% of admissions into a trauma unit (1). It occurs in 0.5%–8.0% of adult trauma patients (2). In paediatric patients, it is estimated to occur at a rate of 4%–6%, and its presence has been reported to indicate high impact. It is associated with other severe injuries in 44%–94% of cases (3). Traumatic diaphragmatic injuries are usually caused by blunt abdominal trauma or penetrating injuries (2); they were first described by Ambriose Paire in 1579 (4). Due to their rarity in infants and children, such injuries can be overlooked if unsuspected. Delayed presentation can lead to life-threatening complications as a result of organ herniation and strangulation (3). Subjects and Methods The study included children (1–18 years old) with traumatic diaphragmatic rupture (TDR) who were admitted to the Department of Pediatric Surgery of Pt BD Sharma Post Graduate Institute of Medical Sciences, Rohtak, Haryana, India, between 1993 and 2005. The following information was recorded for each patient: age, gender, duration between the trauma and hospital admission, type of injury, clinical/radiological findings, relevant information regarding traumatic site, herniated organs into the thorax, associated injuries, and patient’s outcome. Results In the study duration, 11 patients were treated for TDR in our hospital; 8 boys and 3 girls. Their ages ranged from 1–18 years (mean 9.5 years). The TDR occurred following blunt trauma in 9 cases and a penetrating injury in 2 cases (elaborated in Table 1a, b, c). Road traffic accidents were the most common cause. The most common clinical findings were respiratory distress and abdominal pain. All of the ruptures occurred on the left side. The ruptures were localised in the posterolateral parts in 10 cases and near the oesophageal hiatus in 1 case. Eight of the patients were admitted soon after the trauma, while 1 patient was admitted after 7 days of injury. One patient was referred to our hospital after 10 days of injury with bilious contents from the thoracic drainage site (admitted to a peripheral hospital in the initial days following the injury). The chest tube had been inserted into the stomach because it was thought to be a case of hydropneumothorax. Another patient presented with abdominal pain after 1 year of trauma with the small and large bowels herniated into the thoracic cavity. The large bowel had strangulated and required resection and anastomosis. Abnormalities were found in all of the chest X-rays (Figure 1), and all included an elevated or indistinct diaphragm or pleural effusion. Computerised tomography (CT) scan confirmed a diaphragmatic injury with herniation of the abdominal contents in all cases (Figure 2). After adequate investigations and resuscitation, all of these cases were treated surgically through an abdominal approach. The defect was localised, the abdominal contents were reduced, and the defect in the diaphragm was repaired. Post-operatively, all patients had an uneventful recovery with the exception of 2 cases of post-operative bronchopneumonia, which was managed medically. Discussion The diaphragm is a complex, musculotendinous, dome-shaped structure dividing the thoracic and abdominal cavities. In blunt trauma, a diaphragmatic rupture occurs when intra-abdominal forces overcome the normally higher intrathoracic pressure and the elasticity of the contracted diaphragm. The diaphragm most frequently tears at the junction of the muscular and tendinous elements that is called the centrum tendinosum (5). Herniation of the stomach, small and large intestines, kidneys, and spleen may follow the rupture acutely or years after the original injury. Delayed herniation of the abdominal viscera may occur under a number of circumstances. In some cases, the diaphragm weakens secondary to the aggressive inflammatory response at the ruptured site. Patients are also at risk just after tracheal extubation when the intrathoracic pressure quickly becomes negative. Alternatively, visceral content herniation may occur slowly, as the physiologically negative intrathoracic pressures gently pull the abdominal contents through the diaphragmatic defect (6). Most diaphragmatic ruptures occur on the left side. This is believed to be due to a congenitally weaker left haemidiaphragm and the protective effect of the liver on the right side (5). In our study, all of the cases were left-sided. While the classic physical signs of diaphragmatic herniation include unilateral breath sounds, a scaphoid abdomen, and bowel sounds over the lung fields, these clues are not consistently present. Many victims simply demonstrate respiratory distress as their sole pulmonary finding. Additionally, 90% to 95% of individuals with diaphragmatic ruptures have other significant injuries. The most common associated pathologies include lacerations of the spleen, liver, and kidney; pelvic fractures; major vessel disruption; long bone fractures; and head trauma (7). Diaphragmatic injury following blunt trauma remains rare in children and may be more difficult to assess than in adults for both anatomical and physiological reasons. The compliance of the paediatric chest wall may result in internal injury in the absence of the external evidence of major injury (8). As minor injuries have caused ruptures of the diaphragm, the timing of the impact during the respiratory cycle is possibly more important than the severity of the trauma because it creates a significant pressure gradient across the diaphragm. Chest X-ray is one of the most important methods for the detection of diaphragmatic rupture and herniation. The chest X-ray, however, is diagnostic in only 25% to 50% of cases (9). Suggestive findings on the chest X–ray include an interrupted, indistinct, or elevated haemidiaphragm, bowel loops or air-fluid levels in the lung space, and a displaced nasogastric tube into the chest. Rib fractures, pneumothoraces, haemothoraces, lower lobe collapse, and pleural effusions are associated complications that are usually evident on plain films and may increase the suspicion of a more extensive injury (9). Other imaging modalities that are available to the emergency physician to assess the integrity of the diaphragm include ultrasonography (USG) and CT scan (7). Diaphragmatic discontinuity, diaphragmatic thickening, segmental nonrecognition of the diaphragm, intrathoracic herniation of the abdominal viscera, elevation of the diaphragm, and both haemothorax and haemoperitoneum are strong predictors of a blunt diaphragmatic rupture (10). As diaphragmatic tears do not close spontaneously, a diaphragmatic rupture requires surgical closure (5). Laparotomy is the favoured surgical approach to acute diaphragmatic rupture, given that approximately 50% of patients with blunt diaphragmatic injuries have other intra-abdominal pathologies (9). Thoracotomy is commonly employed to repair chronic ruptures. Successful surgical and bioprosthetic repair of TDR poses a serious challenge for surgeons. With the advent of molecular tools, proteomics, regenerative medicine and systems biology, surgeons, physicians, molecular biologists and bioengineers are now following a common translational path to reach a viable solution for successful tissue and organ reconstruction. To the best of our knowledge, there has not yet been a report of any mechanical strain-induced expression of a tendon-specific protein that leads to a visible phenotypic effect in traumatic rupture that contributes to traumatic diaphragmatic herniation. Neither is there any data available that substantiates gene or protein expression in traumatic diaphragmatic hernia or associated multi-organ complications. New strategies ranging from laparoscopic patch and intestinal sub-mucosa to stem cell and tissue-engineered bioprosthetic construct-based strategies for the repair and reconstruction of diaphragmatic hernias have been attempted in several laboratories around the world (11–15). However, most of the data for these types of studies come from congenital cases, and these remain challenging options because of high complication rates. Ongoing and future experiments in animal models for developing foetal cell-based therapies will open newer avenues towards developing a translational approach to successfully deal with traumatic diaphragm reconstruction in children. Conclusion TDR, though uncommon, does occur and should remain a diagnostic possibility in children because these patients do not undergo self-healing and require surgical correction of the defect. It should remain a possibility even in cases of remote trauma, as exemplified by one of our patients who presented after one year of trauma. A CT scan is the best imaging modality because it clearly depicts the anatomy with 3-dimensional reconstructions and highlights other associated organ injuries, which is extremely helpful in treating the patient. Stem cells and tissue-engineered bioprosthetics, which are being tested in several laboratories around the world, can be more relevant in such cases as they can better integrate into growing tissues. Authors’ Contributions Conception and design, statistical expertise: DBD References
© Copyright 2011 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj11008t1c.jpg] [mj11008t1b.jpg] [mj11008f2.jpg] [mj11008f1.jpg] [mj11008t1a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}