 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 18, No. 1, 2011, pp. 52-59 Original Article Factors Affecting the Outcomes in Children Post-Myelomeningocoele Repair in Northeastern Peninsular Malaysia Badrisyah IDRIS Department of Neurosciences, School of Medical Sciences, Universiti Sains Malaysia Health Campus, 16150 Kubang Kerian, Kelantan, Malaysia Correspondence: Dr Badrisyah Idris, MBBChBAO (Ireland), AFRCS (Ireland), MS Neurosurgery (USM), Department of Neurosciences, School of Medical Sciences, Universiti Sains Malaysia Health Campus, 16150 Kubang Kerian, Kelantan, Malaysia, Tel: +609-767 6300 Fax: +609-767 3833 Email: docbdr@yahoo.ie Submitted: 13 Jan 2010 Code Number: mj11009 Abstract Background: The present study aimed to evaluate the impact of multiple factors
and outcomes (ambulatory function and sphincter function) on children with
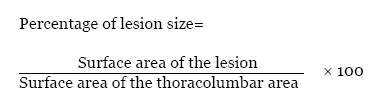
myelomeningocoele (MMC) following surgical repair. Keywords: children, myelomeningocoele, neural tube defects, neurosurgery, spina bifida, spinal cord Introduction Myelomeningocoele (MMC) is the most common congenital disorder of the central nervous system. It is characterised by an exposure of the nervous system and/or meninges to the environment because of a congenital bone defect (1). Children with MMC who survive are likely to have life-long disabilities. Functional problems may often result from the neurologic defect or the surgical repair. In addition, the functional problems may be sequelae of the neurologic deficit (1). The present study was performed to evaluate the impact of multiple factors that are associated with MMC on the outcomes that follow repair. Subjects and Methods Children with MMC that were operated on at the neurosurgical unit of the Universiti Sains Malaysia teaching hospital over a 15-year period (from January 1990 to December 2004) were analysed in the present study. Only those children who were followed-up for at least 18 months after the operation were included in the study. The clinical records of all of the children with MMC were reviewed for information about sex, the mode of delivery, the parental age when the child was born, the size of the lesion, associated abnormalities, the integrity of the MMC sac, the type of imaging performed, the level of the lesion, the time point of the repair of the lesion (duration between the time of diagnosis and repair), the presence of a ventriculoperitoneal shunt, the presence of complications, and the neurological outcome based on the Spina Bifida Neurological Scale (SBNS). Ruptured lesions were defined as any lesions with a ruptured sac, which was usually accompanied by leakage of the cerebrospinal fluid. The percentage of the size of the defect in relation to the thoracolumbar region was calculated using the following formula (2):
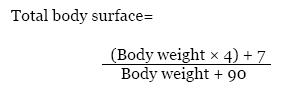
The whole body surface of each patient was determined using the following well-known formula to calculate the total body surface:
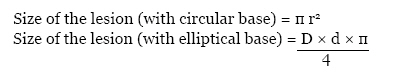
The size of the lesion area was calculated using the following formulae:
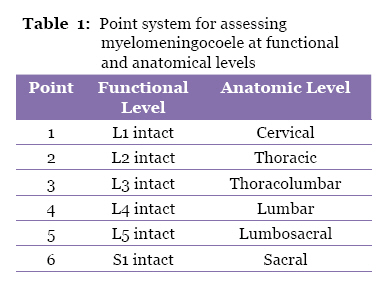
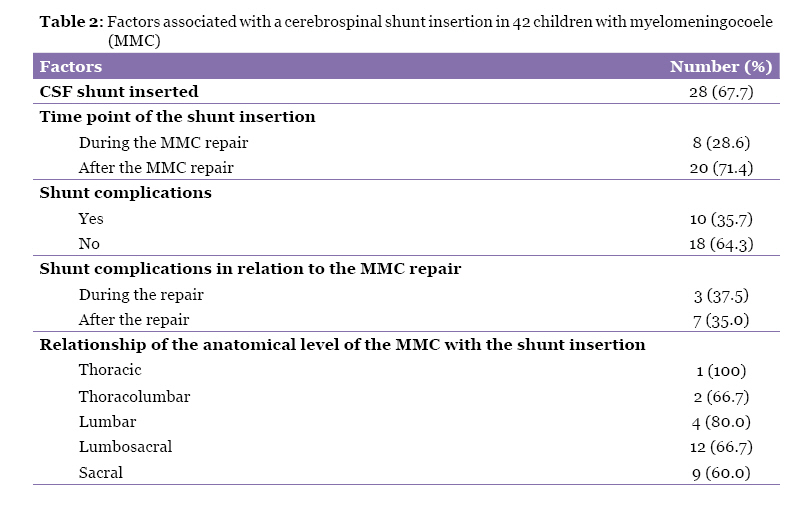
where r is the radius, D is the long diameter, and d is the short diameter. The total areas of the thoracic and lumbar regions were calculated according to the “rule of nines”, which states that these regions constitute 18% of the total body surface. Lesions that occupied less than 8% of the area of the thoracolumbar region were classified as Grade I, and the lesions that occupied more than 8% were classified as Grade II. The level of each lesion was established on the basis of both the anatomical and functional levels. The anatomical level of the lesion was defined as the level of the intact posterior vertebral arch above and below the lesion on the abdominal plain radiograph, taken as a part of the ventriculoperitoneal shunt assessment or the micturating cystourethrogram. In a number of cases, the anatomical level of the lesion was determined from either the magnetic resonance imaging or the computed tomography of the spine. The functional level was determined from the lower limb motor assessments in the neurosurgical, orthopaedic, or paediatric clinic follow-ups. This level was defined as the lowest level of the intact myotome with a power of at least 3/5 on either the right or the left side. Both the anatomical and functional levels were designated by the use of 6-point scale (Table 1). The two methods of assessment were compared by subtracting the anatomical level from the functional level. A negative value indicated that the functional level was higher than the anatomical level and vice versa. The neurological outcomes of the children who had operations for spinal dysraphism were evaluated using the SBNS at 18 months post-repair. The scoring was based on the motor function, reflexes, and bladder and bowel functions; these scores are divided (according to the level of spinal function) into 6, 4, and 5 points, respectively. The clinical status is divided into 5 Grades. Spina bifida Grade I represents a normal spinal neurological function, spina bifida Grade II represents conditions in which there is a voluntary control of bladder and bowel functions, spina bifida Grade III represents problems with ambulation, spina bifida Grade IV represents a non-ambulatory function, and spina bifida Grade V indicates a bedridden status. The main outcome was defined as the ambulatory status at 18 months after the operation. Children who were in Grades I to III were deemed to be ambulant, and those in Grades IV and V were deemed to be non-ambulant. The presence of urinary and faecal incontinence was also analysed as a part of the outcomes. Data entry and analysis was conducted using the Statistical Package for Social Sciences (SPSS) version 15 for Windows (SPSS Inc., Chicago, IL). The comparisons were made between the groups using the Chi-square and Fisher’s exact tests, as appropriate, for the categorical variables and dichotomous outcomes. P < 0.05 was considered to be statistically significant. The associations between the ambulatory status, urinary and faecal incontinence, and significant independent variables from the univariate analysis were analysed with multiple logistic regressions that were adjusted for possible confounding factors to determine the significant variables. The final model of the factors determined using multiple logistic regressions was examined for fitness using the Hosmer–Lemeshow goodness-of-fit test. All results were expressed as odds ratios (ORs) and 95% confidence intervals (CIs). Odds ratios were used to assess the risk of the outcome (ambulatory status and urinary and faecal incontinence) if a certain factor is present. The odds ratio was considered significant if the 95% confidence interval did not include an odds ratio of one. Results The present study led to the review of 78 cases of children that had operations for MMC at our hospital from January 1990 to December 2004; however, only 42 cases were included in the study. The other 36 cases were not analysed due to an absence of follow-up records at 18 months or more after the repair of the MMC. The included cases were comprised of 18 boys (42.9%) and 24 girls (57.1%) with a male to female ratio of 3:4. The mean (SD) birth weight of the children was 3.29 (0.36) kg, and the mean (SD) age of the mothers was 30.65 (5.64) years. The mean (SD) size of the lesions was 17.30 (15.30) cm2. Approximately 88% of the lesions (n = 37) belonged to Grade I, and 12% (n = 5) of the lesions were Grade II lesions. There was no relationship between the Grade of the lesion size and the wound complications (P = 0.618 by Fisher’s exact test). The anatomical levels of the lesion included 1 (2.4%) thoracic lesion, 3 (7.1%) thoracolumbar lesions, 5 (11.9%) lumbar lesions, 18 (42.9%) lumbosacral lesions, and 15 (35.7%) sacral lesions. The functional levels of the cases at 18 months or more post-repair were found to be intact at L1 in 4 cases (9.5%), L2 in 5 cases (11.9%), L3 in 8 cases (19%), L4 in 7 cases (16.7%), L5 in 2 cases (4.8%), and S1 in 16 cases (38.1%). The functional level was higher than the anatomical level in 57.1% of the cases, and the functional level was lower than the anatomical level for only 23.8% of the cases. In 19.0% of the cases, there was no difference between the functional and anatomical levels. From the 42 patients, 34 (81%) were delivered via the vaginal route and 8 (19%) were delivered via Caesarean section. Seventy-four percent of the ruptured MMC cases, and 93% of the unruptured MMC cases, were delivered by the vaginal route. It was found that the mode of delivery was not related to the frequency of the rupture of the MMC (X2 = 2.320, P = 0.128). There were 27 (64%) cases of the MMC rupturing at birth, and 14 (52%) of these cases were repaired within 72 hours. The Grade I lesion size was found to have a significant association with the frequency of sac rupture (P = 0.047 by Fisher’s exact test). Hydrocephalus was found in 71.4% (n = 30) of the patients. The incidence of hydrocephalus was independent of the anatomical (Fisher’s exact = 1.820, P = 0.874) and functional levels of the spinal dysraphism (Fisher’s exact = 5.431, P = 0.354). The presence of hydrocephalus was not a factor that predicted wound breakdown following MMC repair (X2 = 0.840, P = 0.359). Of the 42 patients reviewed, 28 (67.7%) were shunted. Table 2 depicts the factors that were associated with the insertion of a cerebrospinal fluid shunt in these children. The time point of the shunt insertion for hydrocephalus was not related to the time point of the MMC repair (X2 = 1.193, P = 0.223) or to the integrity of the MMC sac (Fisher’s exact = 0.565, P = 0.912). There was no relationship between complications associated with the shunt and the time point of the MMC repair (X2 = 0.016, P = 0.615). Complications related to the surgical wound, such as wound dehiscence, cerebrospinal fluid leaks, and wound infections, developed in 5 patients (14.3%). Sepsis and shunt complications occurred in 2 (4.8%) and 10 (23.8%) patients, respectively. Approximately 5% (n = 2) of the patients had normal neurological function (Grade I), 16.7% (n = 7) of the patients were ambulatory but had bowel and bladder problems (Grade II), 52.4% (n = 22) of the patients were ambulatory but spastic (Grade III), 21.4% (n = 9) of patients were non-ambulatory (Grade IV), and 4.8% (n=2) of patients were bedridden (Grade V). There were 13 (31%) areflexic cases, 15 (35.7%) cases with patellar tendon reflex, 12 (28.6%) cases with ankle reflex, and 2 (4.8%) cases with intact anal reflex. There was no association between reflex functioning and the anatomical level of the lesion (Fisher’s exact = 12.394, P = 0.433). None of the patients with intact functional levels above L2 were ambulatory, whereas 88.2% (n = 15) of the patients with intact L2 to L5 levels and 100% (n = 16) of those with intact S1 and below levels were ambulating 2 years after repair. The significant positive factors for the ambulatory status at 2 years after repair included the presence of hydrocephalus (X2 = 5.961, P = 0.013), the presence of a cerebrospinal fluid (CSF) shunt (X2 = 7.452, P = 0.005), intact motor functions at L3 and below (X2 = 21.917, P < 0.001), and the presence of deep tendon reflexes (X2 = 33.246, P < 0.001). No difference was observed between the ambulatory and non-ambulatory groups in terms of the mode of delivery, the presence of a ruptured sac, the level of the lesion, the time point of the repair, and the size of the MMC. Using multiple logistic regression analyses, no significant associations were established between the main effects of each of the significant predictors and the ambulatory function of the children with MMC 2 years following repair. No interactions were found among the significant predictors. Thirty-five (83.3%) of the children had urinary incontinence, and 18 (42.9%) of the children had faecal incontinence 2 years post-MMC repair. Only 7 (16.7%) of the children had a normal sphincter. Significant associations were observed between sphincter dysfunction and hydrocephalus, occurring in 20 (83.3%) patients (X2 = 3.889, P = 0.049), and low-level MMC (lumbosacral and sacral), occurring in 22 (91.7%) patients (Fisher’s exact = 5.657, P = 0.028). From the multivariate analysis, only the presence of hydrocephalus remained significant in the model for sphincter function. Discussion MMC is the most severe form of a neural tube defect. Its incidence varies between countries and geographical areas. Epidemiological data about this defect from South East Asia are available for 2 cities, Kuala Lumpur and Jakarta. It is predicted that the incidence of neural tube defects in Kuala Lumpur and Jakarta is 2.4 per 1000 and 1.5 per 1000 live births, respectively (3). Because MMC has strong environmental factors in its aetiology, it will be necessary to determine the pattern, aetiological factors, associated anomalies, and factors that affect the outcome in children that have had operations for spinal dysraphism in the Hospital Universiti Sains Malaysia. There was a mild female predominance (female to male ratio of 3:4), which is in agreement with Faraji et al.’s study (4). The majority of MMC are located in the lumbosacral or sacral areas; very few MMC are located at cervical or upper thoracic levels (5). In the present study, 78.6% of MMC were located in the lumbosacral and sacral level. Another study by Rintoul et al. also demonstrated a similar distribution of the level of the MMC (6). Maternal age has an insignificant effect on the incidence of MMC. When a correlation can be found, the risks tend to be higher in older or very young mothers (4,7). In the present study, the youngest mother was 18 years old, and the oldest mother was 40 years old. Large skin lesions can lead to difficulties in the primary closure of the skin, leading to skin necrosis. This study revealed wound complications in 14.3% of the cases. In other series, wound complications ranged from 12% to 22.4% of the cases (8). Appropriate skin flaps and techniques can decrease the wound-related complications (9). In a published study, the authors suggested that a broad base MMC lesion that was more than 8% of the total body surface of the thoracolumbar region should be repaired with muscle-skin flaps, and that those less than 8% of the total body surface of the thoracolumbar region should be repaired primarily (2). Luce and Walsh reported that lesions with a mean area of 22.7 cm2 could be primarily closed, whereas those with a mean area of 37.3 cm2 needed skin grafting for closure (10). Our study found that MMC with less than 8% of the total body surface area of the thoracolumbar region had a higher incidence of rupture. We theorised that a smaller sac was more likely to dry quickly following birth; therefore, increasing the pressure of the CSF that was pooling underneath the dried sac might contribute to sac rupture in small MMC. MMC repair can be performed safely up to 72 hours after birth. This allows for a full assessment of the newborn to identify any associated abnormalities. Ventriculitis had been found 5 times more frequently in infants who underwent delayed MMC closure than in those that underwent a closure that was not delayed (1). One study found that 75% of the cases developed a shunt infection and that the mortality was 13% (11). In the present study, 51.9% of the ruptured MMCs were repaired within 72 hours. Theoretically, the functional level of the lesion should correspond to the anatomical level of the spinal lesion from a radiological examination. However, a retrospective study noted that the functional level was higher than the anatomical level in 48% of individuals and that it was lower than the anatomical level in 14% of individuals (6). Data from our study showed that the functional level was higher than the anatomical level in 57.1% of the children and that it was lower than the anatomical level in 23.8% of the cases. The mode of delivery may have effect on the neurological outcome in children with MMC. The use of a Caesarean section has been advocated as being superior to vaginal delivery in preventing further neurological insult in foetuses diagnosed with MMC antenatally. It has been postulated that the mechanical forces of labour and vaginal delivery may aggravate any already compromised exposed nerve roots (12). This study did not find a significant relationship between the mode of delivery and the ambulatory status in children that had an operation for spinal MMC. Cochrane and colleagues found no association between the mode of delivery and the ambulatory status, except for the neonates that presented as breech. For breech neonates, the authors theorised that neurological damage may occur with vaginal delivery (13). Some authors found that the MMC sac would rupture if the diameter of the sac was more than 4 cm during labour (14). In the current study, the size of the MMC was not associated with rupture of the sac. In another study, the authors found that an elective Caesarean section before the onset of labour might result in an improved neurological outcome in foetuses with MMC, normal karyotypes, and a lack of severe hydrocephalus (15). In a large study that compared elective Caesarean sections to trials of labour, there was no significant relationship between the mode of delivery and the ambulatory status. The authors concluded that the theory that labour causes placode injury was not supported, and injury to the MMC would still take place regardless of the mode of delivery (12). Earlier studies revealed the presence of a Chiari II malformation in nearly 90% of all children with MMC. However, some studies suggested that this malformation was only clinically significant in 10% to 20% of these children who were aged 3 months or less (16). In the present study, only 9.4% of the cases were diagnosed with a Chiari II malformation. This low incidence rate might be due to the fact that most of the children did not survive beyond infancy. As a result, they were not alive long enough to exhibit symptoms that are associated with a Chiari II malformation. Hydrocephalus is the most common abnormality associated with MMC. Prior to the advent of shunting devices, the leading cause of death in children with MMC was uncontrolled hydrocephalus. Previous publications reported that the incidence of hydrocephalus varied from 35% to 90% (9). In the present study, 71.4% of the children with a MMC had hydrocephalus. Almost 87% of those patients with hydrocephalus had a shunt inserted. The present study revealed that for the majority of the cases (71.4%), the shunts were inserted following a repair of the MMC. Hydrocephalus may be worsened following repair because of a loss of the decompressive effect that results from cerebrospinal fluid leakage via a ruptured MMC, because of a loss of the damping effect on elevated intracranial pressure by a bulging MMC sac, and because of further impaction of a Chiari II malformation due to an acute loss of cerebrospinal fluid during operation (5). Cerebrospinal fluid shunts have allowed at least 75% of the children that are born with a MMC to reach their early adult years (17). The timing of the ventriculoperitoneal shunt insertion in relation to the timing of the repair of the MMC remains controversial. Insertion of a shunt simultaneously with a back closure has raised concerns regarding the general susceptibility to infection because of the poor immune function in neonates with MMC. It has been argued that insertion of a shunt reverses the flow of the cerebrospinal fluid from the ruptured MMC in the lumbar region to the ventricles and leads to an infection (18). Many experts advocate simultaneous MMC repair and ventriculoperitoneal shunt insertion to reduce the incidence of cerebrospinal fluid leaks from the operation site and to lead to a shorter hospital stay (19). Alternatively, serial ventricular taps from ventricular access devices may be used initially, and a shunt may be inserted a few days later. Many studies found that comparing the complication rate for shunts that are inserted at the time of MMC repair with those inserted at a later date during a separate procedure did not reveal any differences in terms of shunt infections or shunt malfunctions. Miller and colleagues found that there was a higher rate of cerebrospinal fluid leakage in patients who had ventriculoperitoneal shunt insertion after MMC repair (19). This finding was due to an increased intracranial pressure from the evolving hydrocephalus that resulted in wound breakdown following repair. In a larger study, no difference was observed between the outcome of the shunt function and the time of its insertion in relation to the MMC repair (20,21). Approximately 10% of MMC patients do not require shunt insertion to treat hydrocephalus (18). This study found that 13.3% of hydrocephalic patients did not require shunt insertion. In the present study, shunt complications were not associated with the time point of the repair, the time point of the shunt insertion, and the integrity of the MMC. It has been shown that the frequency of the shunt insertion for hydrocephalus in infants with MMC was associated with the level of the lesion (6,22). A larger number of cephalic lesions were associated with an increased frequency of shunting when assessed at the anatomical and functional level, as demonstrated in the present study. Therefore, foetal repair of MMC might eliminate the need for CSF shunting postnatally. However, there was no significant association between the incidence of shunt insertion and the anatomical or functional level in the present study. These findings were supported by the results from another study that did not find any relationship between the level of the MMC and the incidence of hydrocephalus (4). In 1992, Shizuo Oi and Satoshi Matsumoto proposed a scoring system, the SBNS, that reflects a patient’s clinical status and enables an analysis of the chronological changes of neurological functions (23). This scoring system is an important tool in the follow-up assessment of children who have had an operation for a MMC. This assessment is important because these children may exhibit neurological deterioration as they grow older. In the present study, the SBNS grade was determined 2 years after repair. Due to a lack of data, the pre-operative SBNS grade could not be evaluated. In the present study, 4.8% of the patients had normal neurological functioning (Grade I), 16.7% of patients were ambulatory but had bowel and bladder problems (Grade II), 52.4% of patients were ambulatory but spastic (Grade III), 21.4% of patients were non-ambulatory (Grade IV), and 4.8% of patients were bedridden (Grade V). Another study that used the SBNS grade to evaluate the neurological outcome of patients with spina bifida found 21.8%, 12.7%, 40%, 10.9%, and 14.5% of the cases belonged to Grades I, II, III, IV, and V, respectively (4). In addition paralysis in the lower extremities, almost all individuals with MMC suffer from some degree of urinary and faecal incontinence. Incontinence affects the quality of life of children with MMC. In the present study, 83.3 % of the children did not attain acceptable bladder and bowel continence. The presence of hydrocephalus and a MMC that was located at the lumbosacral or sacral area were strongly associated with poor sphincter control. Similar findings were reported in another published study (24). The ambulatory status in patients with spinal dysraphism is an important factor for functional independence. Children with low-level lesions (low lumbar and sacral levels) are usually able to walk; however, they may need the help of braces and/or crutches. Patients with midlevel lesions (midlumbar level) typically require significant support in the form of braces, twister cables, crutches, or walkers to walk for even brief periods. Most patients with lesions at the upper lumbar level and above require wheelchairs for mobility (25). In the present study, 73.8% of the patients were ambulant at 2 years after the repair of the lesion. The present study demonstrated similar findings in which none of the patients with highly functional lesions could ambulate, and a majority of the patients with intermediate and low-functional lesions could ambulate (88.2% and 100%, respectively). The present study found that the presence of hydrocephalus and CSF shunts, intact motor functions at L3 and below with the presence of knee and ankle reflexes, and a motor level that was lower than the anatomical level were significantly associated with ambulation. By using a multivariate logistic regression, however, none of the odds ratios remained significant in the model. The present study, therefore, agrees with an earlier publication that found that the presence of shunted hydrocephalus, the number of shunt revisions, and the lesion level seemed to be less important with regard to ambulation (26–28). Other authors found several significant predictors of ambulatory status in children with spinal dysraphism. However, comparisons among these studies are difficult because different definitions were used for the level of the lesion and varying classifications were used for the ambulatory statuses (29). It has been suggested that ambulation early in life is a better than the neurological level in predicting the ambulatory status in adult life (30). Another study found that children with a high level of spina bifida who participated in a walking program during early childhood had fewer fractures and pressure sores and were more independent than those who were wheelchair-bound early in life (31). Most studies found that children with thoracic and high lumbar lesions were non-ambulatory (28). Those children who had sacral lesions were able to walk around the community. Children with MMC at other levels were not uniform in terms of the status of their ambulation (28). The present study found a similar pattern in terms of the relationship of the functional level of the lesion and the ambulatory status. It has been reported that hydrocephalus and its complications influence the intelligence of these individuals and affects their ability to recognise their potential to become mobile (28). The present study found a significant correlation of hydrocephalus and shunt insertion with the ambulatory status in the univariate analysis, but the factors was not significant in the multivariate analysis. Conclusion The present study demonstrated that various factors can affect the outcome of children with MMC. Because these children may develop neurological impairment as they grow older, a measuring tool such as the SBNS should be used to monitor any neurological dysfunction. In addition, a multidisciplinary team approach should be employed in the management of children with MMC. Aggressive treatments that prevent further complications should be used to facilitate socially acceptable levels of functional independence in these individuals. References
© Copyright 2011 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj11009t2.jpg] [mj11009t1.jpg] |
| |||||||||

{kind=link}
{kind=link}