 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
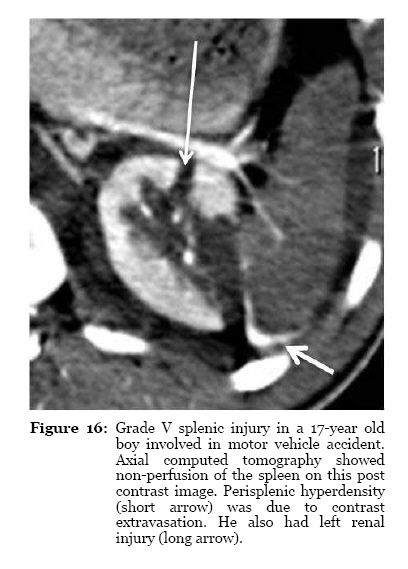
Malaysian Journal of Medical Sciences, Vol. 18, No. 1, 2011, pp. 60-67 Brief Communication Computed Tomography of Blunt Spleen Injury: A Pictorial Review Radhiana HASSAN, Azian ABD AZIZ, Ahmad Razali MD RALIB, Azlin SAAT Department of Radiology, Kulliyyah of Medicine, International Islamic University Malaysia, 25200 Kuantan, Pahang, Malaysia Correspondence: Dr Radhiana Hassan
MD (USM), MMed Rad (USM),
Department of Radiology, Kulliyyah of Medicine,
International Islamic University Malaysia ,
Bandar Indera Mahkota,
25200 Kuantan,
Pahang, Malaysia,
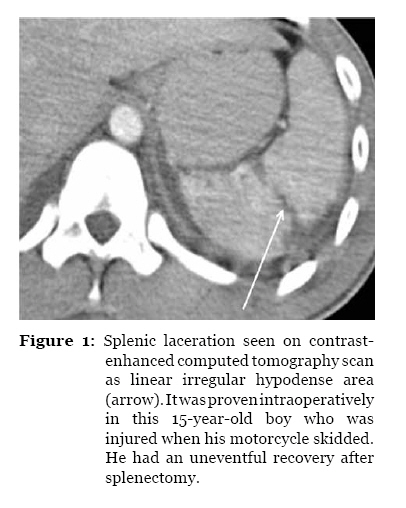
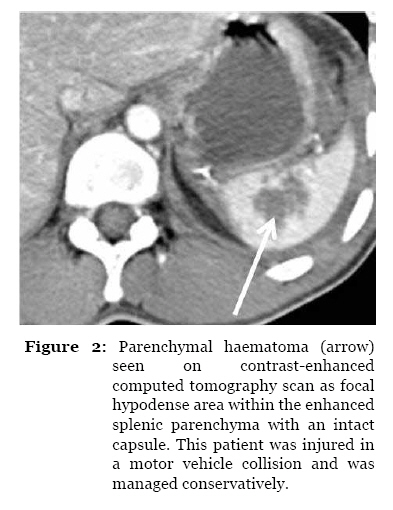
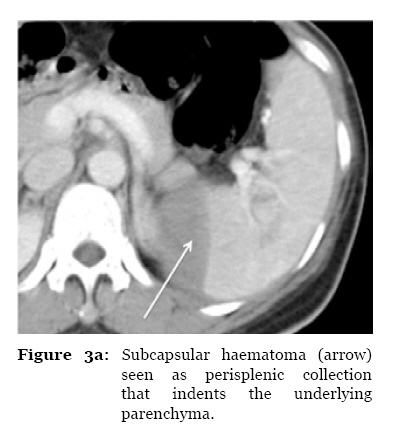
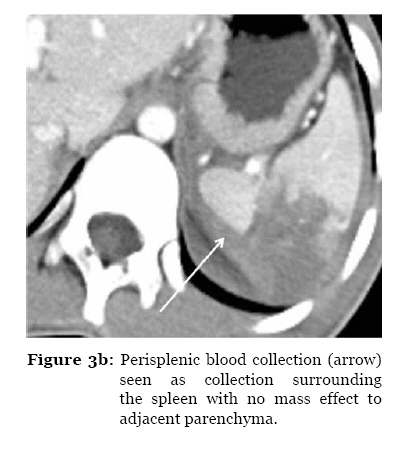
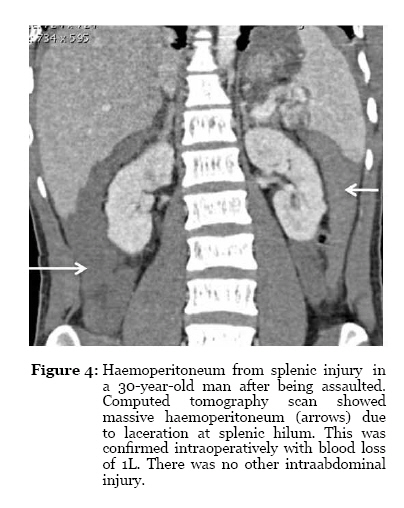
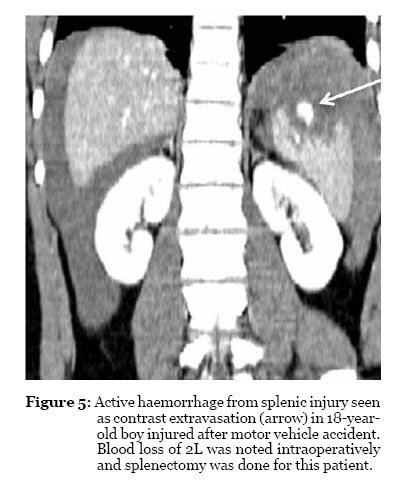
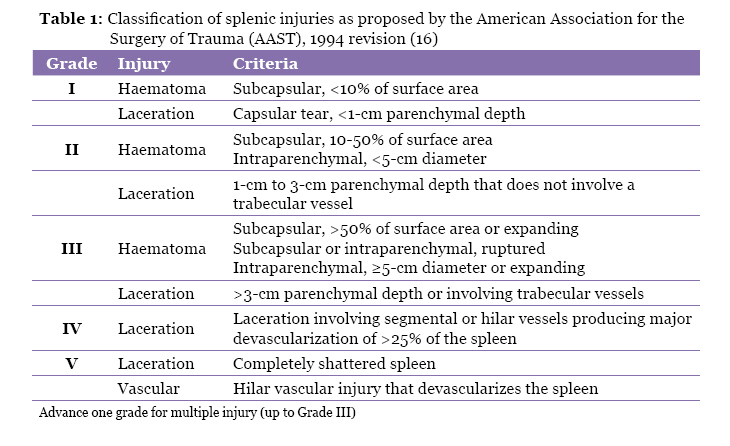
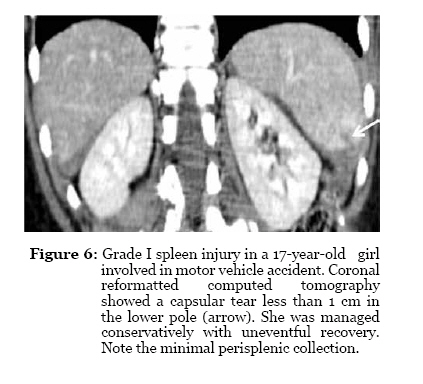
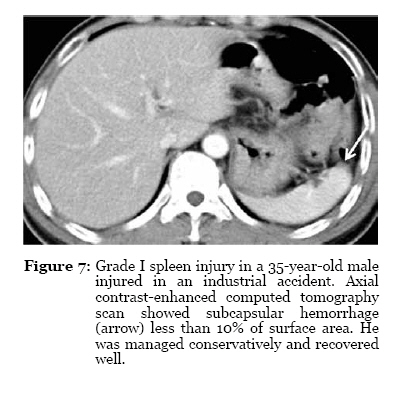
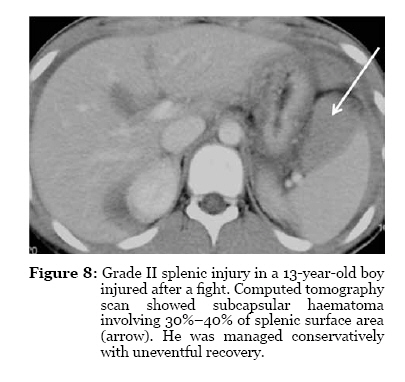
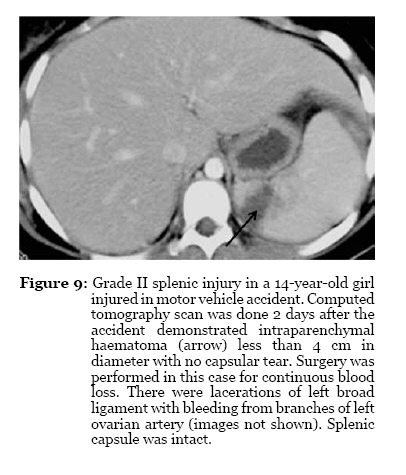
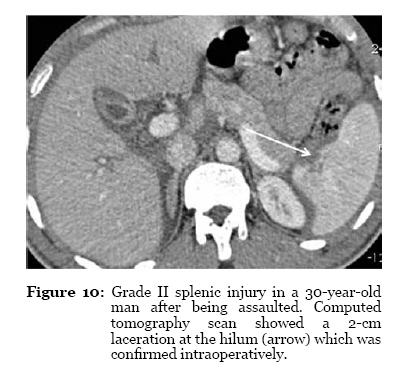
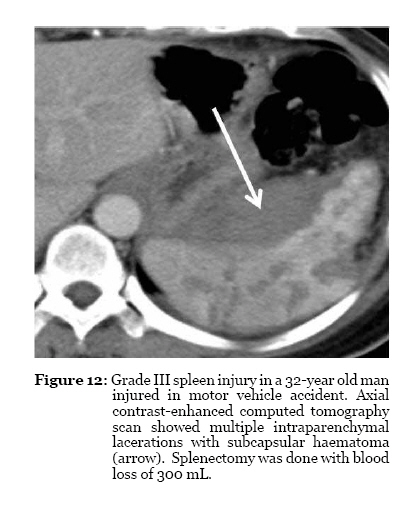
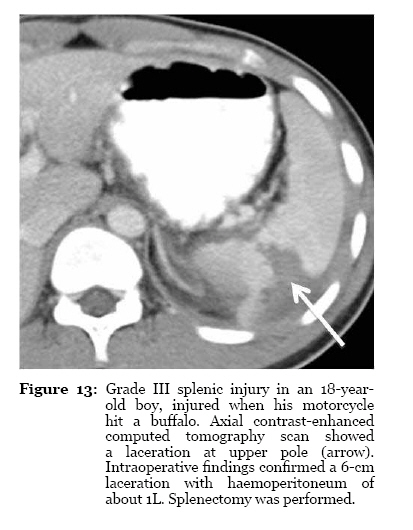
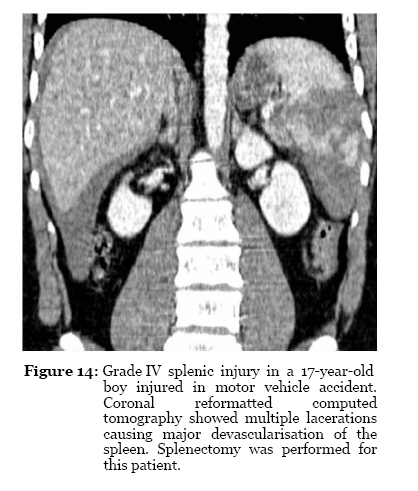
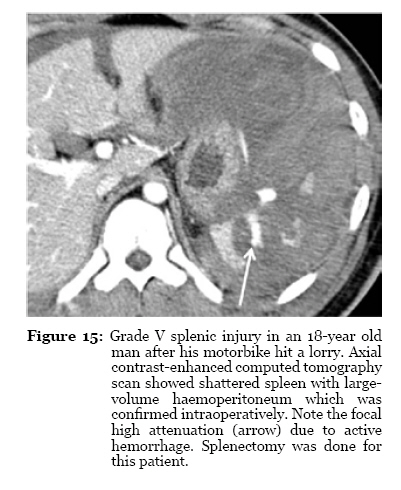
Tel: +609-5572056 Submitted: 7 Jul 2010 Code Number: mj11010 Abstract The spleen is one of the organs most frequently injured in blunt abdominal trauma. Computed tomography (CT) scanning can accurately detect splenic injury and is currently the imaging modality of choice in assessing clinically stable patients with blunt abdominal trauma. The CT features of spleen injury include lacerations, subcapsular or parenchymal haematomas, active haemorrhage, and vascular injuries. We present a pictorial review of the spectrum of CT findings for blunt splenic injuries. This article will be a useful reference for radiologists and surgeons as CT scan is widely used for the assessment of splenic injuries and contributes to the current trend towards nonsurgical management of this injury. Keywords: abdomen, blunt injuries, computed tomography, medical imaging, spleen, trauma Introduction The spleen is one of the organs most frequently injured in blunt abdominal trauma, accounting for up to 49% of all visceral injuries (1,2). Physical examination and laboratory data are often nonspecific in the diagnosis of splenic injury (3). Contrast-enhanced computed tomography (CT) scanning is currently the diagnostic imaging tool of choice for the assessment of haemodynamically stable patients with spleen injury due to its speed, widespread availability, diagnostic accuracy, and relatively noninvasive nature (4). CT scanning can also provide an accurate appraisal of coexisting abdominal injuries, such as injuries to the retroperitoneum and the abdominal wall, and can exclude the presence of lesions requiring surgery, such as bowel or pancreatic injuries (5). The use of CT scanning has influenced the current trend in the management of spleen injuries towards nonsurgical managements (6,7). Even though the decision to use a surgical intervention is usually based on clinical criteria rather than on imaging findings, data from CT scans frequently increase the diagnostic confidence of surgeons and play an important role in decreasing the frequency of unnecessary exploratory laparotomy (7,8). Over a 2-year period (2008–2009) in our hospital, there were 44 cases of spleen injury out of 151 cases for which an abdomen CT scan was performed for blunt abdominal trauma. All of these spleen injury cases were retrospectively reviewed. Of these 44 cases, 12 patients had Grade I injury, 9 patients had Grade II injury, 11 patients had Grade III injury, 4 patients had Grade IV injury, and 8 patients had Grade V injury. For all patients, the CT scans were performed using a 4-row multislice Somatom Siemens Volume Zoom CT scanner (Siemens Medical Systems, Erlangen, Germany) with a 10-mm slice width, 2.5-mm collimation, 0.75-s rotation time, 15-mm table feed, and 3-mm reconstruction interval. Pre- and post-contrast scans were routinely performed. Patients received 2 mL/kg of intravenous contrast medium (iohexol 300 mg I/mL). Oral contrast agents were not routinely given. The post-contrast scans were acquired during the portal venous phase, approximately 80 seconds after contrast injection. Multiplanar reconstruction (MPR) images in the sagittal and coronal planes were acquired when necessary. In this article, we present a spectrum of the CT findings for blunt splenic injuries. The spleen injury grading system was applied according to the classification system of the American Association for the Surgery of Trauma (AAST). CT Features of Blunt Splenic Injury The major CT features of blunt splenic injuries are lacerations, a non-perfused region, subcapsular and parenchymal haematomas, active haemorrhage, haemoperitoneum and vascular injury. Lacerations and intraparenchymal haematomas or contusions can be clearly observed using contrast-enhanced CT (Figures 1 and 2) (9). Subcapsular haematomas appear as an elliptic collection of low-attenuation blood between the spleen capsules and enhanced splenic parenchyma that causes the indentation or flattening of the underlying spleen margin. Free intraperitoneal blood in the perisplenic space does not cause this effect on the underlying spleen parenchyma (Figure 3a & b) (4). Haemoperitoneum can be accurately detected on a CT scan (10). When a patient is in the supine position, blood from the splenic injury passes via the phrenicocolic ligament to the left paracolic gutter and the pelvis. Blood can also pass into the right upper quadrant (Figure 4). Previously, the volume of haemoperitoneum has been considered to be a predictor of the need for surgery in patients with blunt splenic injury; however, recent reports have detailed the successful nonsurgical management of patients with a large amount of haemoperitoneum (11,12). Active haemorrhage appears as an area of high attenuation on a CT image with Hounsfield units value ranging 85–350 due to extravasated contrast material (Figure 5) (13). Contrast extravasation occurs in approximately 17.7% of patients with splenic injury and is a significant predictor of nonsurgical management failure (2). CT-Based Injury Grading System Various CT-based grading systems have been developed for the assessment of splenic injury, with the goals of standardising reporting, planning appropriate management, and enabling comparisons between institutions and studies. However, none of the grading systems correlates well with the need for surgical intervention (7,11,14). Recently, a better correlation between a newly proposed CT grading system and surgical intervention was achieved if important CT findings such as active haemorrhage, pseudoaneurysm, arteriovenous fistula, and the severity of haemoperitoneum were included in the grading system (15). Radiologists should be familiar with CT-based grading systems to facilitate research and communications with the surgeons. The most widely used CT grading system for splenic injury in trauma patients is based on the AAST scale (Table 1) (16). The injuries covered in this study were categorised as Grade I (Figures 6 and 7), Grade II (Figures 8, 9, 10), Grade III (Figures 11, 12, 13), Grade IV (Figure 14), or Grade V (Figures 15 and 16). CT Features of Delayed Complications There are few complications related to splenic injury. Delayed complications of splenic injury occur at least 48 hours after the initial injury and include pseudocysts, abscesses, pseudoaneurysms, and delayed rupture (17,18). Delayed splenic rupture has been reported to occur in approximately 5%–6% of nonsurgically managed adults. Post-traumatic pseudocysts were reported in 0.44% of splenic injury patients (18). Splenic abscess formation is a rare complication of blunt trauma (Figure 17). However, as the trend towards nonsurgical management continues, this rare complication may become more prevalent. Post-traumatic splenic artery pseudoaneurysm is also a rare complication that may develop after splenic injury of any grade. Role of Follow-Up CT in Splenic Injury Follow-up imaging can provide valuable information about healing patterns (17,19). CT scanning demonstrates apparent complete healing of half of all splenic injuries after 6 weeks. Complete healing of all grades is observed 3 months after injury (20). However, this information has not been shown to significantly influence the management of the injury or affect patient outcome, and thus, follow-up CT scans are not currently recommended (18,21). Conclusion A shift towards nonsurgical management of blunt splenic injury in clinically stable trauma patients has been made possible by the widespread use of CT scanning as the initial imaging evaluation. CT scans accurately depict various patterns of splenic injuries and other associated surgically important findings. Knowledge of CT findings of spleen injury is important for both radiologists and surgeons for optimal patient care. Acknowledgements We would like to acknowledge all staff in the of Radiology, Surgery and Emergency Medicine Departments, Hospital Tengku Ampuan Afzan, and Kulliyyah of Medicine, International Islamic University Malaysia (IIUM), for their continuous effort and assistance in the care and treatment of the patients. The data obtained in this pictorial essay is part of a project funded by the IIUM Research Endowment Fund (Type A). Authors’ Contributions Conception and design, provision of patients, analysis and interpretation of data, final approval of the article: RH, AAA, ARMR, AS Drafting of the article, collection and assembly of the data: RH Critical revision of the article: RH, AAA References
© Copyright 2011 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj11010f3b.jpg] [mj11010f10.jpg] [mj11010f9.jpg] [mj11010f7.jpg] [mj11010f11.jpg] [mj11010f2.jpg] [mj11010f16.jpg] [mj11010f12.jpg] [mj11010f15.jpg] [mj11010f6.jpg] [mj11010f17.jpg] [mj11010f4.jpg] [mj11010f13.jpg] [mj11010f14.jpg] [mj11010f1.jpg] [mj11010f3a.jpg] [mj11010f5.jpg] [mj11010t1.jpg] [mj11010f8.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}