 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 18, No. 1, 2011, pp. 76-78 Case Report Acute Acalculous Cholecystitis after Laparoscopic Appendicectomy that Responded to Conservative Management Chee-Kin HUI 1,2 1Centre for Alimentary Diseases, Endoscopy Centre, Central Hospital, 1 Lower
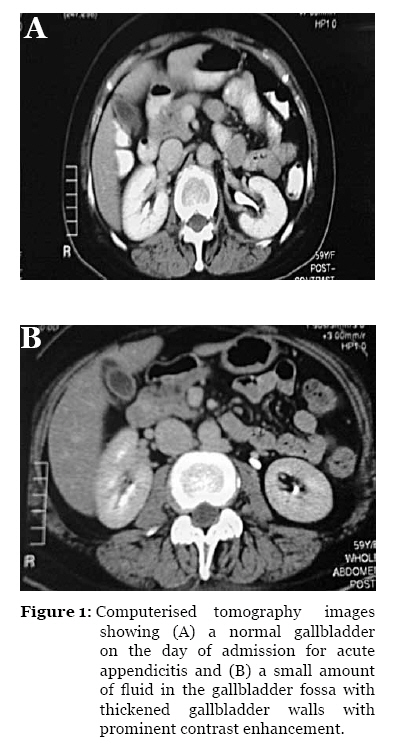
Albert Road, Central, Hong Kong, China Correspondence: Dr Chee-Kin Hui, MD (Hong Kong), Centre for Alimentary Diseases, Endoscopy Centre, Central Hospital, 1 Lower Albert Road, Central, Hong Kong, China, Tel : 852 28671577 Fax : 852 28454730 Email: bckhui@gmail.com Submitted: 30 Jun 2010 Code Number: mj11013 Abstract Inflammation of the gallbladder without evidence of calculi is known as acute acalculous cholecystitis (AAC). AAC is frequently associated with a poor prognosis and a high mortality rate. Thus, early diagnosis and prompt surgical intervention has been recommended to improve the outcome of AAC. Herein, I present a case report of AAC complicating laparoscopic appendicectomy. Unlike previous studies that have reported the need for urgent intervention in patients with AAC, in this study, our patient responded to conservative management. Therefore, the management of AAC after laparoscopic appendicectomy should be individualised. Keywords: acalculous cholecystitis, acute disease, appendicitis, disease management, gut, laparoscopic surgery Introduction Inflammation of the gallbladder without evidence of calculi is known as acute acalculous cholecystitis (AAC). Inflammation of the gallbladder without evidence of calculi is known as acute acalculous cholecystitis (AAC); this condition occurs in 5%-15% of all cases of acute cholecystitis (1). AAC is frequently associated with gangrene, perforation, and empyema. Due to these associated complications, AAC can be associated with high morbidity and mortality (2–3). AAC has been reported in critically ill patients after cardiac surgery, abdominal vascular surgery, trauma, burns, prolonged fasting with or without total parenteral nutrition, sepsis, or atherosclerotic vascular disease (2–3). Here I present a case of AAC arising as a complication of laparoscopic appendicectomy. Case Report A 53-year-old woman with previously good health presented with an acute onset of abdominal pain. The acute abdominal pain initially occurred at the umbilical area and migrated to the right lower quadrant after 12 hours. Examination of the abdomen on presentation revealed tenderness over McBurney’s point with rebound and rigidity. Computerised tomography imaging of the abdomen and pelvis revealed an inflamed appendix in the right iliac fossa with a diameter of 1.5 cm. The appendix had a fluffy border with surrounding soft tissue strands. Wall thickening in the caecum was also present. Laboratory studies performed on admission were unremarkable except for an elevated C-reactive protein (CRP) level of 14 mg/L (normal range less than 10 mg/L). The patient was started on intravenous tigecycline, and a laparoscopic appendicectomy was performed within 2 hours of admission. The procedure was uncomplicated with no episodes of haemodynamic instability during the pre-, intra-, and post-operative periods. Microscopic examination of the appendix revealed features of acute appendicitis, with focal mucosal erosions, suppurative changes, and serositis. The patient resumed a fluid diet on Day 1 post-laparoscopic appendicectomy. As she tolerated the fluid diet well, she resumed a soft solid food diet on Day 2 post-laparoscopic appendicectomy. However, on Day 3 post-laparoscopic appendicectomy, the patient developed right upper quadrant discomfort. Physical examination of the abdomen revealed tenderness over the right upper quadrant, but there was no evidence of rebound or rigidity. Although she remained afebrile, her CRP had increased to 56 mg/L. No other abnormality was detected in the complete blood work-up or in the amylase and liver biochemistry. Computerised tomography imaging of the abdomen was repeated, and a small amount of fluid was seen in the gallbladder fossa. The gallbladder wall was also thickened with prominent contrast enhancement (Figure 1). However, no radiopaque stone was seen in the gallbladder or bile ducts. The common bile duct and the intrahepatic tree were normal in size. No abnormal mass, focal fluid collection or abscess was seen in the right iliac fossa. There was also no abnormal free fluid in the lower abdomen or pelvis. Therefore, based on her right upper quadrant discomfort, right upper quadrant tenderness, the presence of fluid in the gallbladder fossa, and the thickened gallbladder wall with contrast enhancement, she was diagnosed with AAC arising as a complication of laparoscopic appendicectomy. As the patient was haemodynamically stable, she was managed conservatively. In addition to intravenous tigecycline, which had been commenced on the day of admission, the patient was also started on intravenous meropenem and amikacin. On Day 6 post-laparoscopic appendicectomy, her symptoms started to improve. Her CRP on Day 6 post-laparoscopic appendicectomy had decreased to 32 mg/L. On Day 7 post-laparoscopic appendicectomy, her CRP normalised to 9 mg/L. As she remained asymptomatic with a normal CRP, the patient was discharged on Day 14 post-laparoscopic appendicectomy. Her liver biochemistry and amylase levels were normal throughout the course of her hospitalisation. Discussion AAC following surgery was first reported in 1844 (4). Since then, AAC has been reported to occur following cardiovascular surgery, aortic reconstruction, non-biliary tract procedures, and breast reconstruction (5–8). To the best of my knowledge, this is the first report of AAC complicating laparoscopic appendicectomy. The pathogenesis of AAC is postulated to be diverse and has been called “a paradigm of complex inter-relationships” by Barie et al. (9). However, the common denominator for this set of disease states is visceral hypotension (3). As de novo AAC has been reported in healthy patients without any co-existing illness, I believe that in this woman, the AAC complicating laparoscopic appendicectomy was due to biliary stasis that worsened as the result of a spasm of the cystic duct, as postulated by Becker et al. (10). The administration of morphine during the immediate post-operative period may have aggravated the spasm of the cystic duct in this patient (10). AAC is frequently associated with a poor prognosis and a high mortality rate (1,2). Thus, investigators have recommended early diagnosis and prompt surgical intervention to improve the outcome of AAC. However, this recommendation was based on studies in which the subjects had multiple co-morbidities or severe illness, or they were elderly patients (1,2). The patient described in this case report recovered with conservative management and did not require surgical intervention. Therefore, the management of AAC in post-operative patients should be individualised. The clinical condition and pre-morbid condition of the patient must be considered in the formulation of the treatment strategy. In conclusion, this is the first case report of AAC complicating laparoscopic appendicectomy in a patient with no existing co-morbidity. The management of AAC in post-operative patients with no co-morbidity should be individualised. Acknowledgement Special thanks to Dr Alex SY Kwok of The Surgical Department, Dr Vio and Partners Limited, and Dr Wai Kuen Ng of The Department of Pathology, Central Hospital, for their contributions. References
© Copyright 2011 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj11013f1.jpg] |
| |||||||||

{kind=link}