 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 18, No. 2, 2011, pp. 16-26 Original Article Ergonomic Training Reduces Musculoskeletal Disorders among Office Workers: Results from the 6-Month Follow-Up Norashikin Mahmud1, Dianna Theadora Kenny2, Raemy Md Zein3, Siti Nurani Hassan3 1 Program of Industrial and
Organizational Psychology, Faculty of Management and Human Resource
Development, Universiti Teknologi Malaysia, 81310 Skudai, Johor, Malaysia Correspondence: Dr Norashikin Mahmud PhD Health Sciences (University of Sydney) Program of Industrial and rganizational Psychology Faculty of Management and Human Resource Development Universiti Teknologi Malaysia 81310 Skudai, Johor Malaysia Tel: +607-553 6442 Fax: +607-556 6911 Email: norashikin@fppsm.utm.my Submitted: 2 Jun 2010 Code Number: mj11017 Abstract Background: Musculoskeletal disorders are commonly reported among
computer users. This study explored whether these disorders can be reduced by
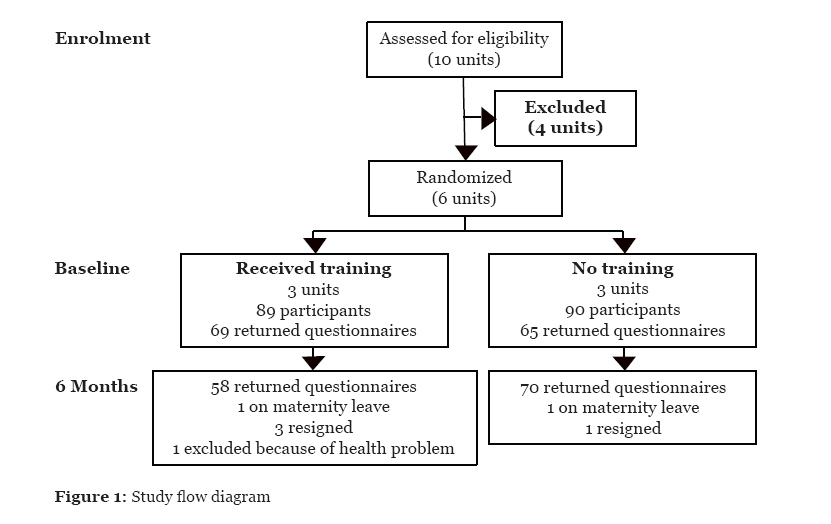
the provision of ergonomics education. Keywords: adult, ergonomics, musculoskeletal diseases, occupational health, training Introduction Musculoskeletal disorders (MSDs) are commonly reported by office workers worldwide, and these disorders can have detrimental effects on workers’ health and productivity (1,2). Factors that predict the risk of developing MSDs can be divided into individual (3–5), ergonomic (6–11), and psychosocial factors (12–15). The risk of developing MSDs is higher among workers who have a high work strain, longer mouse and keyboard use, perceived high muscle tension, and previous MSDs in the neck and shoulder; these risk factors were reported in several longitudinal studies with a follow-up ranging from 3 months to 5.4 years (16–23). Awareness and knowledge of the relationship between computer usage and MSDs are essential for preventing MSDs from becoming more severe. A study conducted by a French company reported that office and blue collar workers had a higher risk of sickness absence because of upper limb disorders compared with managers and professionals (24). A population-based study in Sweden also found that respondents who reported concurrent low back pain and neck-shoulder disorders were at high risk for short- and long-term sickness absences from work (25). In a work setting, ergonomics education/training is the best initial strategy to educate computer users about office ergonomics (26). Training may also educate individuals from different managerial levels in the organisation about office safety, which may simultaneously promote increased levels of safety in the organisation. Previous studies conducted on the effectiveness of office ergonomic training reported improvements in knowledge and workstation habits and a reduction in MSDs. One study used various educational interventions, including posters, emails, pictures of stretching and stress relief activities, workshops, and informational booklets. These interventions increased the workers’ knowledge of cumulative trauma disorders and resulted in changes in the hand/wrist and neck/shoulder posture when using computers (27). The other study conducted on workers in a petrochemical research and development facility reported improvements in workstation posture and symptom severity, but they did not report any reduction in symptoms (28). Studies using different methods of ergonomics training have reported positive results. For example, those who received education programs, such as participatory training (an active learning session involving discussions and problem-solving exercises) and traditional training (lectures and handouts), reported less pain/discomfort and a positive perception of psychosocial work stress compared with those who did not receive training (29). Another study demonstrated that both instructor-directed and self-directed learning were effective in causing positive changes in ergonomic habits among workers (30). However, a study reported that training alone did not reduce MSD symptoms among respondents (31). The researchers suggested that knowledge derived from training would not be effective unless workers were provided with the appropriate equipment to implement it. Recent studies on office ergonomics by Robertson et al. (32,33) also found positive results. One study looked at the effect of 3 interventions, office ergonomics training, a flexible workstation, and training with a flexible workstation, on an individual’s psychological work environment, musculoskeletal disorders, and work effectiveness. In the study, flexible workstation was architecturally designed to create a sense of openness, provide natural lighting throughout the workspace, and enhance auditory and visual privacy. The layout of the individual workstations was a soft U-shape, with each workstation having adjustable storage and paper management tools. Each workstation was equipped with a highly adjustable ergonomic chair. Regarding MSDs, they showed a significant reduction in MSDs in the training with a flexible workstation group (32). Another study aimed to investigate the effects of training and training with an adjustable chair on musculoskeletal risk, knowledge, and behavioural change. An improvement in the observed computing body postures for the right and left side of the body with the training and training with a chair groups. Regarding behavioural changes, only the training group reported a significant improvement in the workstation changes at the time of the follow-up session (33). The aim of the current study was to evaluate the effects of office ergonomics training, compared with no training, on MSDs and psychological well-being in university-based office workers. A cross-sectional survey that assessed their awareness of office ergonomics and the prevalence of MSDs had been previously conducted among the target group of the Universiti Teknologi Malaysia (UTM) office workers. The findings reported a low level of office ergonomics awareness and high 12-month prevalence rates of MSDs in the shoulder (51.6%), neck (48.2%), and back (42.2%) (34). Results from the study suggested that UTM staff were in need of office ergonomics training because they had not previously received any formal training. Two hypotheses were drawn: (1) office ergonomics training reduces musculoskeletal disorders among office workers; and (2) office ergonomics training can improve the psychological well-being among office workers. Subjects and Methods Study design Ethical approval to conduct the study was obtained from the University of Sydney Human Research Ethics Committee. This study was designed as a two-armed cluster randomised controlled trial. The experimental group received office ergonomic training, and the control group was asked to conduct “business as usual” (no ergonomic training); 3 units were randomly assigned to the experimental group, and 3 were assigned to the control group using a random number table. The random number was set at 6. The minimum value was set at 1 (experimental group) and maximum value at 2 (control group). The researchers were aware of the allocation of the groups. Respondents were aware of the study, but they did not know whether they belonged to the experimental or control group. The study flow chart is presented in Figure 1. Participants and setting Office workers from 6 units were invited to participate in the study. The 6 units were Bursary, Registry, Library, Research Management Centre, Professional and Continuing Education, and Centre of Information and Communication Technology. The inclusion criteria were people who worked with computers for at least 3 hours per day, in either permanent or contract employment. The exclusion criteria were people who had any previous illness and/or injuries that may have contributed to MSDs. The majority of the office workers sat in cubicles; the size of the cubicle was standardised, but it may have been smaller for several of the workstations due to space constraints. Each worker had his/her own designated desk equipped with a monitor (traditional or flat screen), a keyboard (traditional), and a mouse (without a wrist rest). The majority of workers working in a cubicle had a keyboard tray (without a mouse tray), which was attached to the desk. Some, but not all, workers who were not working in a cubicle had desks with a keyboard tray. Workers who did not have a keyboard tray placed their keyboard on their desk. Most staff had their own telephone; however, a small number of participants shared a telephone with co-workers (1:2). Chairs and desks were adjustable, and the staff had flexibility with respect to the movement of their keyboard and mouse. Workstation layouts were generally consistent across units. No serious efforts had been made by management to ergonomically upgrade these workstations. The initial awareness of office ergonomics was low (34). Intervention Respondents from the intervention groups received office ergonomics training. The in-house ergonomics training was conducted by trainers from the National Institute of Safety and Health (NIOSH). The training took place over a period of 1 day, divided into 2 sessions; the first session consisted of lectures on office ergonomics, understanding the relationship between office ergonomics and the development of MSDs, ergonomic improvements and adjustments of workstations, and stretching exercises. The second session focused on the practical aspects of the training; trainers visited the participants’ workstations and provided assistance to them on how to adjust workstations effectively. We encouraged respondents to stay at their workstation so that the trainers could help them readjust their workstation if necessary. Trainers made suggestions on how to improve workstation practices, but these were restricted to different arrangements of the workstation furniture without compromising the space available. Respondents were also encouraged to participate in their workstation adjustments. Under some circumstances, further suggestions were made on how to adjust the workstation and/or space. These suggested changes would have required support from management; for example, trainers suggested buying new furniture or allocating more space. Respondents from the control groups received a leaflet that consisted of an ergonomic office diagram, tips on how to take a break, tips on how to reduce their workload, and stretching exercises. The leaflet was based on a comprehensive literature search from the National Institute of Occupational of Safety and Health and other health and safety websites related to office ergonomics issues or problems. The experimental group also received the same leaflet in addition to the ergonomic training. Outcome measures We assessed outcomes at the 6-month time point after training. The primary outcome measure was self-reported MSDs. Respondents were asked if they had experienced any MSDs at any time during the previous 6 months. Musculoskeletal disorders were measured based on 9 categories: neck, right and left shoulder, upper and lower back, right and left upper limbs (upper arm, elbow, lower arm, wrist, and fingers), and right and left lower limbs (thigh/hip, knee, and feet). Data concerning the prevalence of MSDs were gathered using the modified Nordic Questionnaire (35). Workstation habits, psychological well-being, and sick leave were the secondary outcome measures. A sample of the respondents’ workstation habits was randomly selected for observation in each of the 6 units at both baseline and follow-up time points. The observations were conducted by 4 people from the NIOSH. Trial observations were conducted prior to actual observation of 2 office workers to make sure that trainers had a clear understanding of the workstation specification checklist (Table 1) and would use it reliably. The rating was either yes (if the respondents had the desired workstation habits) or no (undesired workstation habits). A strong inter-rater reliability was found between the 4 observers (Cronbach’s alpha 0.844). The checklist included items related to the use of the monitor (5 items), keyboard (7 items), mouse (2 items), chair (7 items), and desk (2 items); for example, some items were as follows: if the monitor is at arm’s length away from the user, if the keyboard is at the right height (elbow height), and if the mouse is placed near the keyboard and within reach. Table 1: Workstation observation checklist
Psychological well-being was measured using the Depression Anxiety Stress Scale (DASS)-21 questionnaire (36). Respondents were asked to evaluate their psychological well-being based on a 4-point scale (0 = did not apply to me at all; 1 = applied to me to some degree or some of the time; 2 = applied to me a considerable degree or a good part of the time; and 3 = applied to me very much or most of the time). Sick leave was assessed by 2 items: “in the last 6 months, how many days (approximately) in total have you had off work due to work-related musculoskeletal discomfort?” and “in the last 6 months, how many separate times have you had time off work due to work-related musculoskeletal discomfort?” Statistical analysis We conducted an intention-to-treat analysis in which respondents were considered for the intervention that was assigned to them, i.e., training and workstation adjustments. Respondents who provided data at baseline and post-intervention time points were included in the analysis. We measured the effect of short-term behavioural changes at 2 weeks post-intervention. The between-group differences for workstation habits were calculated by examining the differences in the mean scores of correct ergonomic habits for the monitor, keyboard, mouse, chair, and desk; an independent t test analysis was used to analyse significant differences between the groups at follow-up. The between-group differences for the rates of MSDs were calculated using percent differences with 95% confidence intervals. Chi-square analysis was used to analyse the significant differences between groups. We then adjusted the P value for the baseline values using logistic regression. We calculated the number needed to treat (NNT) to determine the number of individuals that need to receive the intervention to reduce MSDs. For the analysis of the effect of intervention on sick leave, a Mann–Whitney U analysis was used to determine post-intervention significant differences between groups. An independent t test was used to calculate the mean differences between post-intervention and pre-intervention of psychological well-being scores and significant differences between groups. We used an analysis of co-variance (general linear model) to adjust follow-up values for baseline values for sick leave and psychological well-being. Baseline results for demographic and occupational characteristics The demographic and occupational characteristics of the study population are presented in Table 2. The baseline characteristics between the 2 groups were similar for age, gender distribution, body mass index, psychological well-being, and workplace characteristics. However, a greater number of respondents in the control group completed higher education and exercised less than the experimental group. Respondents who provided data at baseline and post-intervention were included in the analysis. In total, data from 43 respondents in the experimental group and 55 in the control group were analysed (for primary and secondary measures). Table 2: Demographics and occupational characteristics of study population
Data are expressed in mean (SD) or percentage. Abbreviations: INT = intervention, CON = control, BMI = body mass index, SRP = Sijil Rendah Pelajaran (Lower Certificate of Education), SPM = Sijil Pelajaran Malaysia (Malaysian Certificate of Education), DASS = Depression Anxiety Stress Scale. Workstation observations Short-term improvements were observed with intervention in workstation habits in the intervention groups (Table 3); specifically, these improvements were seen with the use of the monitor (mean score = 3.8), keyboard (mean score = 5.4), mouse (mean score = 1.2), chair (mean score = 5.7), and desk (mean score = 1.8) at the follow-up time point. The differences between groups were significant for the keyboard (P = 0.005), mouse (P = 0.042), chair (P <0.0001), and desk (P = 0.033). A marginally significant difference for monitor use was observed (P = 0.063). Conversely, only 1 significant difference for the improvement of workstation habits was recorded in the control group, and it was related to the space needed for the participant’s legs to comfortably fit under the desk and the placement of items on the desk (P = 0.025). Table 3: Workstation habits differences between groups at baseline and 2 weeks post-intervention
Data are expressed in mean score (SD). Self-reported musculoskeletal disorders Summaries of MSDs are given in Table 4. The results show that the percentage of MSDs in the intervention groups was consistently reduced for all outcomes at the follow-up time point and ranged from -10.3% to -44.2%. The largest reduction percentage was for the neck region (-42.2%, 95% CI -60.0 to -24.4), followed by the left upper limb (-29.6%, 95% CI 46.31 to -12.89) and left lower limb (-28.1%, 95% CI -41.99 to -14.21). The lowest reported reduction percentage was for the upper back (-10.3%, 95% CI -28.9 to 8.3), left shoulder (-19.9%, 95% CI -38.4 to 1.4), and right upper limb (-19.9%, 95% CI -39.45 to -0.35). The unadjusted effects for baseline values showed statistically significant lower discomforts in the neck, right shoulder, right and left upper limbs, lower back, and right and left lower limbs. For these regions, NNT was in the range of 2 to 5, which indicated that 2 to 5 people needed to receive the intervention for 1 person to benefit from a reduced musculoskeletal problem. The results on the left shoulder were marginally significant, but the differences between the groups were clinically important and greater than 19%. No statistically significant benefits were observed for the upper back, and the NNT was much higher (10). Table 4: Musculoskeletal disorders at a 6-month follow-up time point (unadjusted and adjusted for baseline) assessed using the modified Nordic Questionnaires
aData are expressed in number of subjects (percentage). bDifference between 6 months of INT and CON in percentage (95% CI). Abbreviations: INT = intervention, CON = control, NNT = number needed to treat, U = unadjusted P value, A = P value adjusted for baseline. Number of days and episodes of sick leave and psychological well-being The unadjusted and adjusted effects of the intervention showed no significant differences between groups for the number and episodes of sick day outcomes (Table 5). Although mean score differences were found between the 2 groups for stress (-0.593, 95% CI -1.7 to 0.5), anxiety (-0.018, 95% CI -1.1 to 1.1), and depression (-0.431, 95% CI -1.5 to 0.7) during the follow-up, these effects were not statistically significant (Table 6). Table 5: Number of days and episodes of sick leave
Data are expressed in mean (SD; range). Abbreviations: INT = intervention, CON = control, U= unadjusted P value, A = P value adjusted for baseline. Table 6: Psychological well-being (stress, anxiety, and depression) as assessed using DASS-21
aData are expressed in mean score (SD; range). bDifference between 6 months of INT and CON in mean score (95% CI). Abbreviations: DASS = Depression Anxiety Stress Scale, INT = intervention, CON = control, U= unadjusted P value, A = P value adjusted for baseline. Discussion The findings of this study suggest that training improved workstation habits with respect to how workers used their monitor, keyboard, mouse, chair, and desk in the intervention group at 2 weeks post-intervention. The largest improvements were found in the workers’ body posture in the back region, thighs, knees, and feet while sitting. Significant improvements were also found regarding the position of the keyboard, workers’ body posture for the elbow, forearms, upper arms, wrists, and shoulders when typing. The differences between groups during the follow-up period were significant for the keyboard, mouse, chair, and desk. Only 1 significant improvement for workstations was found in the control group (i.e., monitor use, space for legs under the desk, and location of items on desk). Our findings are consistent with other studies that have found that ergonomics training improved workstation habits (30,37,38). The intervention group scored consistently lower values for all outcomes during the follow-up, although the difference was not statistically significant for the upper back. The largest percentage reduction was found for the neck, followed by the left upper and lower limbs. This outcome is in agreement with the findings of other studies that reported reductions in MSDs among computer users after attending training (32,38). It was also supported by the fact that the respondents had positive improvements on workstation habits, especially in how they sat and used keyboards, which may reduce the risk of developing neck, back, and other upper extremity disorders. The improvements in MSDs did not translate into fewer days lost from work. We are not sure whether the reduction of MSDs had an effect on the number and episodes of sick leave among workers. We measured a reduction in the symptoms’ frequency but not the severity and duration of pain among respondents. Therefore, it was unclear whether training reduced MSDs and resulted in fewer sick days among respondents. Similarly, intervention had no effect on workers’ psychological well-being. The lack of significant changes on depression, anxiety, and stress, assessed by the DASS-21 questionnaire, may have been due to a floor effect. As a whole, the samples did not demonstrate a significant level of depression, anxiety, and stress at the baseline, and this did not change over the course of the study. Our findings did not agree with the results of Bohr (29), who reported that training improved the health status and reduced the respondents’ psychosocial work stress perceptions among those who received the education programs. The researcher was not sure whether the decrease of psychosocial work stress was caused by the improvement in the work area configuration or the improvement in the worker’s posture. The present study provided evidence that training had a positive impact on the workers’ musculoskeletal disorders at a 6-month follow-up. Several studies conducted on the effectiveness of office ergonomic training on MSDs included a follow-up at 12th month. These studies provided evidence of a long-term positive effect of training on MSDs. The current researchers are also interested in conducting a follow-up at 12th months to determine the impact of training on musculoskeletal disorders, number of days and episodes of sick leave, and psychological well-being. Contamination between individuals from the same clusters may influence the outcome effect. In addition, transfer of knowledge between clusters might occur during social interactions or from workers who were from the same geographical area but in different locations (i.e., buildings). We did not adjust for confounding effects, such as age, years of working with computers, or hours spent typing, in the analysis of the effects of the intervention. Although these confounding effects might influence the outcome, they were fairly well balanced at baseline by the randomisation process. The strength of our study was the randomisation of groups for intervention and control, which is the most efficient way to control for the effects of known and unknown confounding effects. However, blinding the respondents and the researchers could have helped reduced the responder and observer biases. Conclusion The current study was a preliminary report to determine the effectiveness of office ergonomic training to reduce MSDs in UTM. We found that office ergonomic training improved workstation habits and reduced MSDs among office workers. We hope that the results will benefit the UTM staff because they demonstrate to the management that inexpensive ergonomic training had a positive impact on the safety and health of office workers. University management can actively participate in both training and investing in adjustable furniture for office workers. Further research that combines training and the use of adjustable furniture in UTM is recommended in the future. Acknowledgements The authors thank each member of units who participated in the study, and also the Director of Occupational Health and Safety Unit, UTM, who supported our study. We also would like to thank trainers from NIOSH who conducted workstation observations. References
© Copyright 2011 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj11017t4.jpg] [mj11017t1.jpg] [mj11017t3.jpg] [mj11017t2.jpg] [mj11017t5.jpg] [mj11017t6.jpg] [mj11017f1.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}