 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 18, No. 2, 2011, pp. 47-52 Original Article Chemical Composition of Gallstones from Al-Jouf Province of Saudi Arabia Bashir M Jarrar, Meshref A Al-Rowaili Department of Clinical Laboratory Sciences, College of Applied Medical Sciences, Al-Jouf University, PO Box 2014, Saudi Arabia Correspondence: Dr Bashir M Jarrar PhD Histochemistry (Khartoum University) Department of Clinical Laboratory Sciences College of Applied Medical Sciences Al-Jouf University PO Box 2014 Skaka – Al-Jouf Saudi Arabia Tel: +00966- 43647100 Fax: +00966-46257328 Email: bashirjarrar@yahoo.com Submitted: 26 Aug 2010 Code Number: mj11021 Abstract Background:
It is essential to understand the aetiopathogenesis of gallstone disease. This
study was undertaken to determine the chemical composition of gallstones from
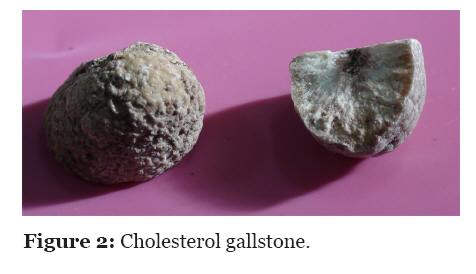
patients living in Al-Jouf Province of Saudi Arabia. Keywords: bilirubin, calcium bilirubinate, cholesterol, clinical chemistry, gallstones, Saudi Arabia Introduction Gallstones have been known to humans for many years and have been found in the gallbladders of Egyptian mummies dating back to 1000 BC (1). Gallstone is one of the diseases prevalent in developed nations, but it is less prevalent in the developing populations that still consume traditional diets (2,3). Gallstones are more common in North America, Europe, and Australia, and are less prevalent in Africa, India, China, Japan, Kashmir, and Egypt, with variable frequency, such as 4.1% in Tunisia, 4.7% in Iran, 5.4% in Bangladesh, 5.4% in Peru, 7.8% in Germany, 20.8% in New Zealand, and 15% in the USA (4–6). Epidemiological studies show that gallstones formation is a complex multifactorial disease associated with dietary habits, overweight, sex, and family history of gallstone disease, with no evidence of racial or climatological factors resulting in the increase in cholelithiasis (3,7,8). The chemical composition and location of the biliary calculi differ in various parts of the world and change over time because of nutritional, socio-economic, and demographic factors (9). Gallstone chemical analysis gives important evidences for the origin, aetiology, and the metabolic basis of its formation, and helps in the identification of risk factors that predispose certain individuals to the calculi formation. Few scattered reports on gallstone disease are available from different parts of Saudi Arabia; the disease prevalence at the country level is increasing, but no thorough study has been conducted (2,8,10–15). Few, if any, reports are available about the chemical composition and the aetiopathogenesis of gallstones in Saudi Arabia. The present study was done to determine the chemical composition of gallstones removed from patients receiving treatment in Al-Jouf Province of Saudi Arabia, and their incidences, as well as to find the association of gallstones with age distribution and lifestyle in an attempt to understand the pathogenesis of cholelithiasis in Saudi Arabia. Materials and methods Chemical analyses were conducted on 46 gallstones from patients in Al-Jouf Province of Saudi Arabia. These stones were removed surgically from January 2007 to January 2008 in the hospitals of Al-Jouf Province. Analyses were carried out at the central laboratory of the Department of Clinical Laboratory Sciences, Al-Jouf University. The relevant patients’ information, namely, age, sex, number of calculi, estrogen therapy, number of childbirths, and family history of cholelithiasis, were obtained from hospitals’ records. The physical parameters of the calculi, such as colour, number, shape, texture, and cross section, were noted. The size was determined by measuring the largest diameter of solitary stones and deducing the average for the multiple stones. The calculi were powdered in a mortar and were analysed chemically by semiquantitative titrimetric and colourimetric methods (16,17). Powdered stones were analysed for cholesterol, bilirubin, triglyceride, calcium, and carbonate. Test solutions were prepared by dissolving 30 mg of powdered stone in 3 mL of chloroform, and the solutions were kept in a water bath at 100 °C for 2 minutes. These stone solutions were used for the determination of total cholesterol and total bilirubin by colourimetric methods (17). In a separate preparation, 30 mg of powdered stone was dissolved in 3 mL of 1 N hydrochloric acid; distilled water was then added to a final volume of 10 mL. The test solutions were kept in boiling water for 60 minutes. These solutions were used for the determination of triglyceride, calcium, and carbonate by titrimetric and colourimetric methods (16). Organic and inorganic nature of the gallstones was identified by flame and burning tests (18). The dissolved stone solutions were stored at 2–6 °C when not in use. The incidence of gallstone was analysed using the number of specific gallstones as the numerator and the number of gallstones extracted (n = 46) as the denominator. The exact confidence interval was calculated using a web-based calculator (http://www.measuringusability.com/Exact.htm). One sample-one tailed Z test was used for comparison of statistical significance, which was defined as P < 0.05 (19,20). Results Out of 46 gallstones of 46 patients, 28 (60.9%) stones belonged to females while 18 (39.1%) belonged to males, giving a male to female ratio of 1:1.6. The age of the patients ranged 19– 75 years, while 19 (41.3 %) patients were in their third decade of life (Figure 1). The hospitals’ records indicated that 38 (82.6%) patients suffered from cholecystitis while 25 (54.3%) had family history of cholelithiasis. Out of 28 female patients, 13 (46.4%) had multiple parity. There were 18 (39.1%) patients with multiple stones, while the rest had solitary stones. Cholesterol stones were soft with smooth surface and showed central radiations on cross sections (Figure 2). Bilirubin stones were soft and amorphous with rough surface, while the mixed stones had rough surface with laminated cross sections (Figure 3). The size of the tested stones varied in diameter (4–62 mm), where 21 (45.7%) of these gallstones measured 25 mm and above. Pure cholesterol stones were bigger in size in comparison with pure bilirubin and mixed stones and were mainly green yellowish, with a few stones that were whitish yellow. The result of the chemical analyses revealed that 56.5% of the stones were pure stones (cholesterol or bilirubin), while 43.5% contained more than one chemical. Table 1 shows the distribution of the types of stones according to the chemical analyses. Table 1: Distribution of stones according to the chemical groups
* 95% confidence interval was calculated by using exact method. Cholesterol was present in 38 (82.6%) stones; it was more frequent in females (n = 24, 63.2%, 95% CI 46.0–78.2) than in males (P < 0.001). The incidence of bilirubin-containing stones (n = 12, 26.1%) was slightly higher in males (n = 7, 58.3%) than in females (n = 5, 41.7%). However, this was not statistically significant (P = 0.240). The triglycerides were seen only in cholesterol and bilirubin mixed calculi. Calcium was seen in 15 (32.6%) of the calculi, and it accompanied cholesterol stones more than bilirubin stones (P < 0.001). Carbonate accompanied calcium in only 7 (15.2%) of the stones, where calcium carbonate was seen mainly in the cholesterol mixed calculi, with 2 (4.3%) stones containing calcium and bilirubin only. Discussion Gallstones represent a major problem in many countries, including Saudi Arabia (21,22). Reports from different parts of the world indicate that the incidence of gallstones is correlated with socio-economic conditions and dietary factors (9,23); other risk factors are marked obesity, family history of gallstone disease, high energy intake, aging, multiple parity, cholecystitis, and sedentary lifestyle (15,24–27). Gallstones are more frequent among patients with certain conditions, such as Crohn's disease and liver cirrhosis (25). Studies in Saudi Arabia showed changes in dietary habits; the average daily individual consumption of the total calories, including fat and sugar, increased, while consumption of high-fibre grain fell (13). This might contribute to an increase in the frequency of cholelithiasis, as cholecystectomy in Saudi Arabia became one of the most common major abdominal surgeries in the Kingdom (13). Consumption of simple sugars and saturated fat has been mostly associated to a higher risk of cholelithiasis (27). Our results showed that females were more affected with cholelithiasis than males, with a female to male ratio of 1.6:1. According to the Central Department of Statistics, Saudi Arabia, female to male ratio of the total Saudi population was 100:102 in 2005 (28). The female predominance of cholelithiasis, as seen in the present study, is in agreement with findings from other provinces of Saudi Arabia, but is significantly lower (P < 0.001) than in Asir Province and Riyadh city (8,15). Reports from other countries, such as in India, Pakistan, Albania, and Jordan, also indicate that females are more affected by the disease than males (21,29–31). This might be due to the basic hormonal differences between males and females, together with the differences that might exist due to co-expression of sex hormone receptors in the gallbladder of both sexes. The medical records of the patients of the present study showed that most of the female patients had parity. This is also in agreement with other studies, which concluded that fertility and multiple pregnancies appeared to be a risk factor for gallstones among Saudi women (15). Increased levels of sex hormones as a result of pregnancy may increase cholesterol in the bile and decrease gallbladder movement, resulting in cholelithiasis. The present investigation showed cholelithiasis in Al-Jouf Province was more frequent among people in their third decade of life. This is in agreement with Murshid’s investigation from Saudi Arabia (15). Investigations concluded lower sensitivity of the gallbladder to cholecystokinin in older human volunteers (aged 60–84 years) in comparison with younger volunteers (aged 22–42 years) after ingestion of Lipomul (1.5 mL/kg) by both groups (7,32). Cholesterol was the most common constituent (82.6%) of the gallstones, followed by calcium, bilirubin, and carbonate in the present investigation. This finding is in agreement with a study in the western region of Saudi Arabia, where 90.4% of the gallstones contained cholesterol (12). Reports from western countries, such as Germany and some Scandinavian countries, also showed cholesterol as the primary component of the gallstones, but different gallstone composition were reported in studies from Sub-Saharan Africa and China (21,33–35). The differences may be attributed to both metabolic abnormalities of cholesterol metabolism and different dietary conditions of the people in these countries. Formation of cholesterol calculi have been related to high carbohydrate diet, which leads to cholesterol supersaturation in the bile (36). Atherosclerosis, hyperlipidaemia, and hyperinsulinism have also been encountered as risk factors for cholesterol gallstone disease (25,26). The association between cholesterol intake and gallstone disease has been indicated by different studies (23,26). The results of the present investigation also indicated that cholesterol-containing stones were less frequent in males than in females (P < 0.001). This is in line with reports from other countries, such as Korea (37). The findings of the present work showed that bilirubin was conjugated with calcium or cholesterol and that the stones occurred more frequently in the mixed forms rather than as pure bilirubin stones. This is contrary to the finding of the chemical analysis of gallstones from India (30). In addition, it has been reported that bacterial infection of the gall bladder helps in hydrolysis of conjugated bilirubin, forming free bilirubin in the form of calcium bilirubinate salt (38). The present work also indicated that gallstone calcium content was highest in bilirubin stones and lowest in cholesterol stones. It has been reported that calcium bilirubinate precipitates in the bile and play a critical role in cholelithiasis (30,39). The hospitals records of Al-Jouf Province indicated that 82.6% of the patients included in the present study had a history of cholecystitis. Injury of the epithelial lining of the gall bladder might be a risk factor for calcium bilirubinate precipitation due to the release of β-glucoronidase (40). The records also showed that 54.3% of the patients had a family history of cholelithiasis. This is in agreement with some reports that correlated gallstone disease aetiology with genetic and environmental factors (27). Conclusion It is apparent from the findings of the present investigation that the most common gallstone in Al-Jouf Province of Saudi Arabia was cholesterol stone, and that the age group at risk of having gallstones was the third decade of life, with a higher risk for females than males. Additional studies are needed to understand the pathogenesis of cholelithiasis in Al-Jouf Province and other parts of Saudi Arabia and to clarify its relation with the lifestyle, especially the dietary habits. Acknowledgement Special thanks are given to Dr Wael Elayat for his help in the chemical analyses of the gallstones utilised in the present work, and to Yazun Jarrar for his help in the statistical analyses. References
© Copyright 2011 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj11021f1.jpg] [mj11021f3.jpg] [mj11021f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}