 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 18, No. 2, 2011, pp. 70-73 Case Report The Value of Pre-Operative Embolisation in Primary Inferior Vena Cava Paraganglioma Faizah Mohd Zaki1, Syazarina Sharis Osman1, Zaleha Abdul Manaf2, Jeyaledchumy Mahadevan2, Mazri Yahya3 1Department
of Radiology, Universiti Kebangsaan Malaysia Medical Centre, Jalan Yaacob
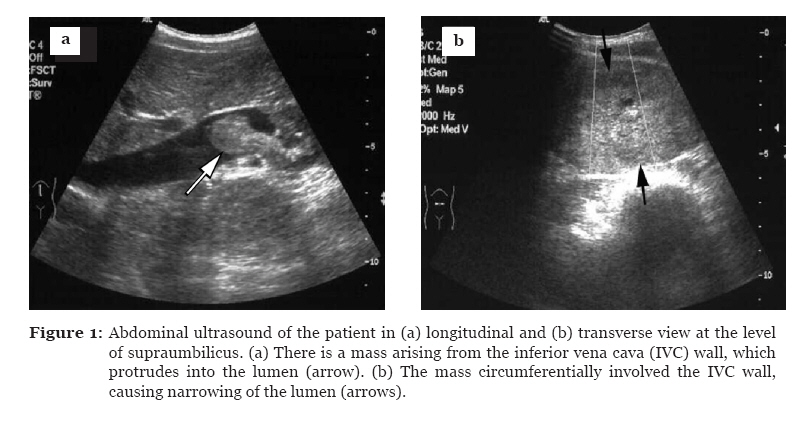
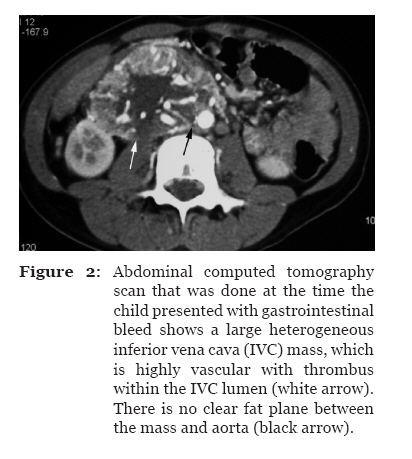
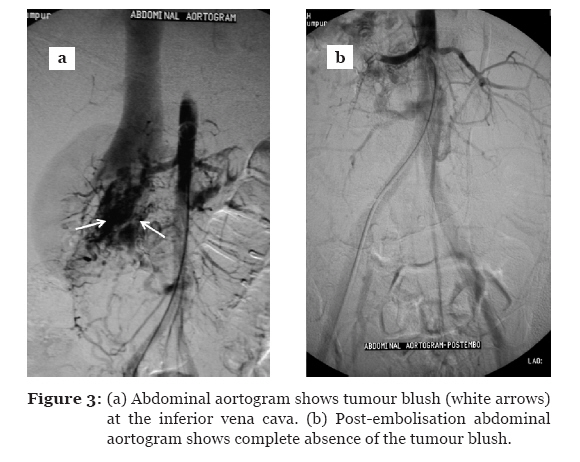
Latiff, Cheras, 56000 Kuala Lumpur, Malaysia Correspondence: Dr Faizah Mohd Zaki MD (UKM), MMed Radiology (UKM) Department of Radiology Universiti Kebangsaan Malaysia Medical Centre Jalan Yaacob Latiff 56000 Cheras Kuala Lumpur, Malaysia Tel: +6019-273 7282 Fax: +603-9173 7824 Email: faizahbangi@yahoo.co.uk Submitted: 11 Aug 2010 Code Number: mj11025 Abstract We report a case of a 13-year-old boy who complained of progressive abdominal distension and symptoms of anaemia. Radiological investigations revealed that the child had a hypervascular tumour of the inferior vena cava (IVC). Unfortunately, the child presented with acute lower gastrointestinal bleed soon after the investigation. He underwent an urgent pre-operative embolisation, aimed to reduce the tumour vascularity. A total resection of the tumour, right nephrectomy, and partial duodenal resection were done within 24 hours post-embolisation. The child was stable post-operatively. The histopathological examination revealed chromogranin-positive paraganglioma originating from the IVC. We highlight the radiological findings of rare primary IVC paraganglioma and the role of embolisation prior to surgical removal of the tumour. Keywords: children, inferior vena cava, paraganglioma, radiology, therapeutic embolisation Introduction Primary tumours originating from blood vessels are rare. They almost exclusively arise from veins and most commonly originate in the inferior vena cava (IVC). Their histology is almost exclusively leiomyosarcoma (1). Therefore, paraganglioma is even rarer to originate from IVC, as it is a tumour of neuroectodermal origin and classified as extra-adrenal paraganglioma. A study done in a large paediatric cancer centre over a 22-year period showed that extra-adrenal paraganglioma constitutes only 0.034% of the patients evaluated for non-haematological malignancy (2). Unfortunately, both IVC tumours and paragangliomas are largely vascular tumours, which makes pre-operative tissue diagnosis and complete surgical clearance challenging and, possibly, mutilating (3). This case report discusses the imaging features of a rare cause of IVC tumour and the value of pre-operative embolisation of the tumour supply prior to operation. Case Report A previously healthy 13-year-old boy presented with a 3-month history of lethargy and shortness of breath, with associated progressive abdominal distension. He was found to be anaemic in his initial blood investigation; he was then transfused with packed cells. There was no associated symptom of high catecholamine, such as hypertension or tachycardia. Initial computed tomography (CT) scan showed an IVC tumour. A presumptive diagnosis of IVC tumour was made, and he was referred to our institution’s vascular team for further management. The issue of pre-operative biopsy was discussed at length. A detailed ultrasound of the abdomen with Doppler study was done to assess the vascularity of the tumour. It showed a circumferential mass within the IVC wall. It was highly vascular and demonstrated a floating intraluminal thrombus (Figure 1). Based on the vascularity of the tumour, an ultrasound-guided biopsy with interventional and surgical backup was planned. He was allowed home leave before the planned high-risk procedure. Unfortunately, the child developed malaena and haemetemesis at home, with associated symptoms of anaemia. An urgent CT scan of the abdomen was done to rule out intra-abdominal gastrointestinal bleed due to tumour invasion. It showed a huge IVC tumour with intraluminal thrombus (Figure 2). In view of the active gastrointestinal bleed, pre-operative angiography was performed with an anticipation of embolising the major feeding vessels. Pre-embolisation anatomy revealed major feeding vessels from the 3 right lumbar arteries and ileocolic branch of the superior mesenteric artery (SMA); 2 of the lumbar arteries and the SMA branch were successfully embolised with gold particulates (EmboGold) using a 4Fr microcatheter. Post-embolisation films showed marked reduction in the vascularity of the lesion (Figure 3). Pre-operative diagnosis at that time was IVC tumour, most likely leiomyosarcoma. The child underwent laparatomy 1 day after the embolisation. Intra-operative findings showed an intraluminal IVC tumour that was densely adhered to the right kidney as well as the second and third part of duodenum. The right ureter was wrapped by the tumour and displaced laterally. Therefore, the whole tumour was dissected away from the aorta and resected. Right nephrectomy and resection of the second and third part of duodenum were done. Sutures closed both ends of the IVC stump. There was minimal intra-operative blood loss (less than 1 litre). The post-operative period was uneventful, and the child was discharged after Day 15, when oral feeding was well tolerated. Histopathological examination was reported as IVC paraganglioma with positive chromogranin. There was no evidence of invasion of the right kidney or the adherent duodenum. There was also no evidence of metastatic lymph nodes in the specimen. The child was well upon follow-up at 1 month after discharge. Discussion Paragangliomas are rare neural crest neoplasms arbitrarily classified by their relationship to the adrenal gland. Adrenal-medullary tumour (phaeochromocytomas) occurs 9–10 times more often than the extra-adrenal paragangliomas (2–4). The most common sites of extra-adrenal paragangliomas are the para-aortic region at the level of renal hila (46%), at the organ of Zuckerkandl (29%), thoracic para spinal region (10%), bladder (10%), and head and neck (2%–4%). Paragangliomas may be multicentric, manifesting as unilateral or bilateral lesions, and occurring synchronously or metachronously (3). Extra-adrenal paragangliomas are more likely to be malignant (40%) than adrenal phaeochromocytomas (2%–11%). It can be associated with several familial syndromes, including multiple endocrine neoplasia type 2A and type 2B, neurofibromatosis type 1, and Carneys triad (2,4,5). These tumours secrete epinephrine and norepinephrine, which clinically result in hypertension, headaches, sweating, and palpitations (2,6). The biochemical diagnosis is aimed in determining catecholamine levels (epinephrine, norepinephrine, and dopamine) as well as their 24-hour urine metabolites, which was found to be around 90% sensitive (7). The patient did not have any catecholamine symptoms,which made the diagnosis of paraganglioma was not suspected prior to surgery. The urine catecholamine test was not performed in this patient, as he did not show symptoms of high catecholamines pre- and post-surgery. Tekautz et al. (2) reviewed 8 paediatric patients (mean age of 11.4 years) with extra-adrenal paraganglioma and reported that urine catecholamine test was not done routinely in these cases. In his review, urine catecholamines were measured in only 1 patient after operation when he was hypertensive post-operatively, whereby the results were within the normal limits. Extra-adrenal paragangliomas, by virtue of their rarity, are less described with regard to the imaging features. Extra-adrenal paragangliomas have nearly identical imaging features, including a homogenous or heterogeneous hyperenhancing soft-tissue mass at CT, multiple areas of signal void interspersed with hyperintense foci (salt–pepper appearance) within tumour mass at magnetic resonance imaging (MRI), and an intense tumour blush with enlarged feeding arteries at angiography (5). Sahdev et al. (4) described that 13 of the 15 cases of extra-adrenal paraganglioma in their series showed heterogeneous masses on CT and MRI, with avid enhancement. There was central necrosis, but with avid peripheral enhancement in the larger tumour section, as in this case. The study concluded that the large retroperitoneal paragangliomas demonstrated no unique features on CT and MRI. Their appearances overlapped with the reported appearances of other retroperitoneal tumours, particularly neurofibromas, neuromas, and sarcomas. Angiography of the tumour prior to operation helps to provide information concerning vascular supply of the tumour, patency of the arterial supply of the surrounding organs (i.e., bowels and kidneys), and allows subsequent pre-operative embolisation, which is valuable for pre-operative planning. Most tumours are hypervascular and have blood supply from more than one artery. The primary vessels supplying these tumours are the lumbar arteries. In addition, other vascular supplies of the tumour are the celiac, mesenteric, or renal arteries (8). Bourke et al. (3) reported a case of a retroperitoneal paraganglioma that received vascular supplies from 3 lumbar arteries and a right lower pole renal vessel. Our patient had arterial supply from the lumbar arteries as well as superior mesenteric artery. Pre-operative embolisation is a useful procedure to optimize operative conditions as it allows avoidance of excessive intra-operative blood loss and possible injury to nearby structures from poor operative field visualization (3). Experienced interventional radiologist is needed to plan the degree and timing of intervention; this is to avoid complications in the child, such as pain and infection. Bourke et al. (3) suggested that embolisation is best undertaken within 24 hours of expected definitive operation. In fact, our patient underwent the surgical debulking of the IVC tumour within 24 hours post-embolisation, with an excellent result of complete resection and minimal blood loss. In conclusion, the long-term outcome of paragangliomas can be difficult to predict, but complete surgical resection gives the best chance of long-term cure (3). Despite of absence of high-catecholamine symptoms, such as hypertension, the diagnosis of paraganglioma need to be considered in a retroperitoneal tumour, which then warrants further biochemical investigation. Even though there is no specific imaging feature for retroperitoneal IVC paraganglioma, CT scan and MRI would help in planning the plane of the tumour with surrounding structures. In addition, angiography helps in terms of identifying the feeding vessels with definitive pre-operative embolisation of the feeding arteries, which will reduce the risk of intra- and post-operative morbidity. References
© Copyright 2011 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj11025f1.jpg] [mj11025f3.jpg] [mj11025f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}