 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 18, No. 2, 2011, pp. 78-81 Case Report A Rare Case of a Subcutaneous Phaeomycotic Cyst with a Brief Review of Literature Madhavan Manoharan1, Natarajan Shanmugam2, Saveetha Veeriyan3 1 Department of Pathology, Saveetha Medical College, Thandalam,
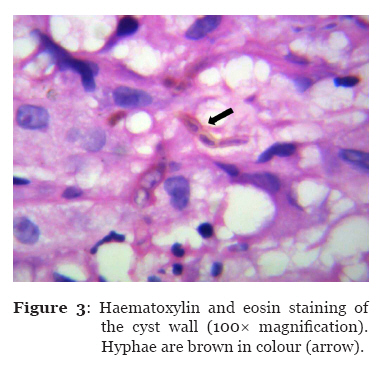
Kanchipuram District, India, 605102 Correspondence: Associate Professor Dr Manoharan Madhavan MBBS (University of Madras), MD Path (Pondicherry University) Saveetha Medical College Thandalam, Kanchipuram District India, 605102 Tel: +91-90-9403 3599 Fax: +91-44-2681 1171 Email: madhavan6@gmail.com Submitted: 31 Aug 2010 Code Number: mj11027 Abstract Phaeohyphomycosis consists of a heterogeneous group of fungal infections caused by more than 80 genera and species. Subcutaneous infection usually follows traumatic implantation of a fungus by a wooden splinter that the fungus inhabits as a saprophyte. The growth of the fungus forms verrucous plaques or a painless subcutaneous abscess. We report a subcutaneous cyst (phaeomycotic cyst) in the leg of a 60-year-old woman that developed after a thorn prick at that site. With the provisional diagnosis of an epidermoid cyst, she was treated with a simple excision of the cyst. However, histopathological examination of the cyst revealed the typical features of fungus, and a definitive diagnosis of a phaeomycotic cyst was made. As the infective aetiology was not considered clinically, the specimen was not sent for microbiological culture, and hence the exact species was not identified. As the lesion was localised, simple excision was sufficient treatment, and no recurrence was observed during 12 months of follow-up. Keywords: clinical microbiology, cyst, dermatomycosis, diagnosis, female, leg dermatoses Introduction Phaeohyphomycosis is a heterogeneous group of fungal infections caused by a variety of naturally pigmented fungi. The aetiological agents of this mycosis, which include more than 80 genera and species, are common saprophytes found in soil, wood, and decaying vegetable matter (1,2). Phaeohyphomycosis is rare, although it is more common in immunocompromised individuals (3). Phaeohyphomycosis affects either superficial tissues, such as the skin, cornea, and subcutaneous tissue, or deep tissues, such as the brain, and cases of phaeohyphomycosis are classified accordingly (2). Subcutaneous infection is usually caused by Exophiala and Phialophora species (4). The infection typically follows traumatic implantation of the fungi by a wooden splinter or a thorn prick and manifests as a cystic lesion. Herein, we report a typical case of a subcutaneous phaeomycotic cyst occurring in an elderly woman. Case Report A 60-year-old woman presented with painless swelling over the anterior aspect of the right leg for the past one and half years. It started as a small swelling and gradually reached the present size. The patient, a labourer, was pricked by a thorn while clearing wild bushes two years ago. Swelling was noticed a few months after the incident. On examination, her general condition was good. She was afebrile. Other systemic examination results were within normal limits. Local examination revealed a firm, fluctuant, mobile swelling measuring about 3 × 3 cm situated over the anterior aspect of the right leg. It was not painful or tender. It was not attached to the underlying bone. An X-ray of the right leg showed a well-circumscribed soft tissue nodule in the subcutaneous plane in the anterior aspect of the shin (Figure 1). The underlying bone appeared normal, with no abnormal lytic or sclerotic lesions or cortical breaks. The chest roentgenogram was normal. Her haemoglobin level was 9.0 gm/dL, sugar 82 mg/dL, urea 34 mg/dL, and creatinine 1.0 mg/dL. The urinalysis results were normal. Operative findings The soft tissue mass was easily separated from the surrounding tissue and was removed in toto. When the excised cyst was cut open in the surgical theatre, it expelled purulent material (Figure 2). The cyst was immersed in 10% formalin and sent for histopathological examination. Histopathological examination Microscopy revealed a fibrocollagenous cyst wall lined by granulomas, composed of foreign-body giant cells, epithelioid cells, xanthoma cells, and lymphoplasma cells. Some of the giant cells contained fungal hyphae. The hyphae were pigmented (Figure 3) and septate. Constrictions were present at a few septations, forming a structure similar to a bamboo stem (Figure 4). With these histological characteristics, the diagnosis of a phaeomycotic cyst was made. As the specimen was preserved in formalin, fungal culture to identify the species could not be performed. Follow-up The suture was removed after 2 weeks, and the wound healed well. There was no recurrence observed during the 12 months of follow-up. Discussion Phaeohyphomycosis infections occur worldwide in both animals and humans. These infections are more common in immunodeficient or debilitated hosts and rarely affect healthy individuals (3). Phaeohyphomycosis has been clinically divided into superficial (cutaneous and corneal), subcutaneous, and systemic phaeohyphomycosis by McGinnis (2). Subcutaneous phaeohyphomycosis is usually caused by Exophiala and Phialophora species (4). Occasional cases caused by Fonsecaea species have also been reported (5). Subcutaneous phaeohyphomycosis usually results in a painless subcutaneous abscess or in verrucous plaques on the hand, arm, face, or neck. Although phaeohyphomycosis has distinct clinical features, it is occasionally confused with chromoblastomycosis (Table 1). Table 1: Clinical differences between chromoblastomycosis and phaeohyphomycosis
Typically, phaeohyphomycosis follows traumatic implantation of the fungus by a wooden splinter, as in our case. Lymphangitis and regional lymphadenopathy are unusual. Hence, infective aetiologies are usually not considered. Our case was clinically suspected to be an epidermoid cyst. The host reaction to phaeohyphomycosis is similar regardless of the aetiological agent and the anatomic site of involvement. The lesion is usually situated in the dermis and the subcutaneous plane and is characterised by cyst formation with dense collagenous connective tissue and central suppurative necrosis. The overlying epidermis is usually normal. The wall contains compact aggregates of epithelioid histiocytes and numerous giant cells. Pigmented moniliform fungal elements are usually present inside the giant cells or extracellularly in the necrotic debris. Fungi may vary in their degree of pigmentation and may also appear as infrequently branching hyphae measuring 2–6 mm wide. The fungi are closely septate and constricted at their prominent septations (3). Our case exhibited the typical features of phaeohyphomycosis. In many cases, identification of the exact species is not attempted, as phaeohyphomycosis is not suspected clinically. Similarly, in our case, an infective aetiology was not suspected, and after excision in the operation theatre, the cyst was fixed in formalin. When culture and identification of species is not pursued, the cyst can be histologically differentiated from black grain eumycotic mycetoma (Table 2) and chromoblastomycosis (Table 3). Table 2: Histological differences between black grain eumycotic mycetoma and phaeohyphomycosis
Table 3: Histological differences between chromoblastomycosis and phaeohyphomycosis
Regarding the management of subcutaneous phaeohyphomycosis, excision of the localised lesion is usually curative (6). In our case, after the local excision, there was no recurrence found during the 12 months of follow-up. Conclusion Subcutaneous phaeohyphomycosis is a rare fungal infection caused by a wide variety of dematiaceous fungi. A high index of suspicion for infective aetiologies is needed to make a proper clinical diagnosis. For a localised lesion, simple excision is usually curative. When phaeohyphomycosis is not suspected and the identification of species by culture is not pursued, routine histopathological examination is sufficient to arrive at a diagnosis of phaeohyphomycosis. Acknowledgement We sincerely thank the Medical Director, Saveetha Medical College Hospital, and the Vice Chancellor, Saveetha University, for allowing us to submit this case for publication. References
© Copyright 2011 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj11027f1.jpg] [mj11027f4.jpg] [mj11027f2.jpg] [mj11027f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}