 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
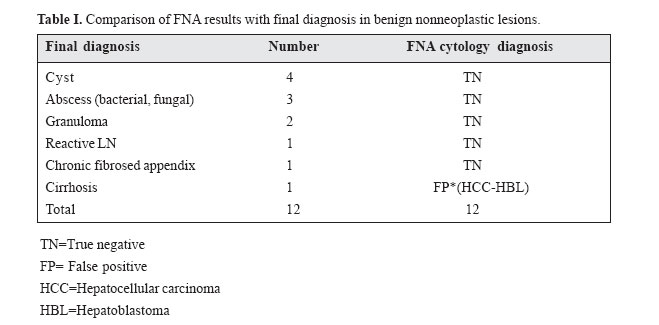
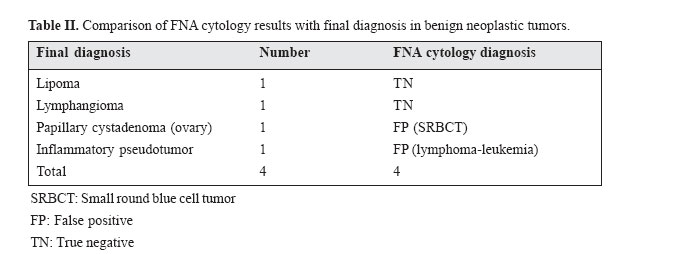
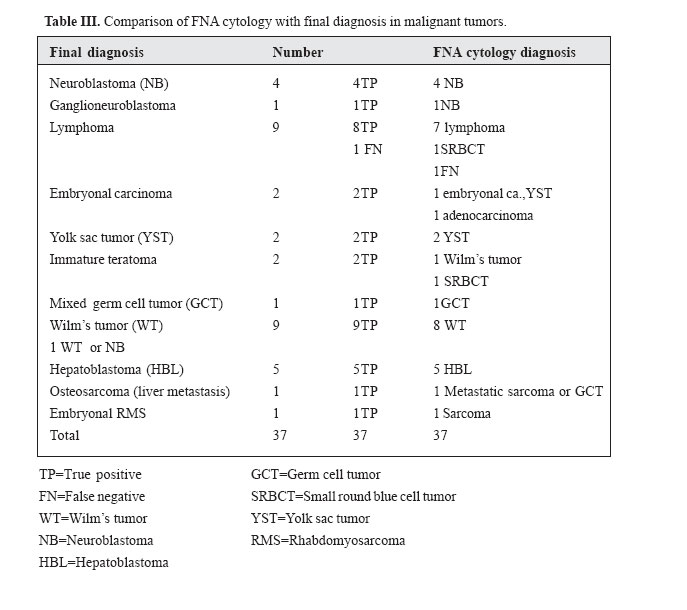
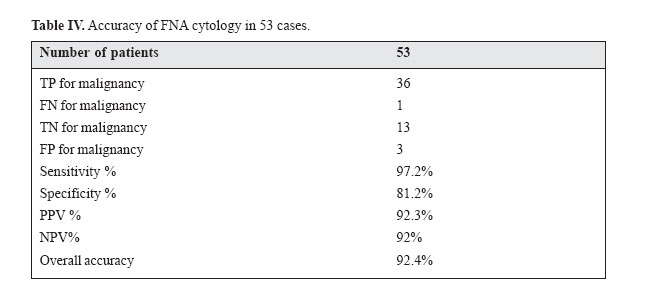
Medical Journal of the Islamic Republic of Iran , Vol. 18, No. 1, May, 2004, pp. 29-33 VALUE OF FINE NEEDLE ASPIRATION IN DIAGNOSING ABDOMINALAND RETROPERITONEAL MASSES OF CHILDREN B. GERAMIZADEH, A. AZIZI, P.V. KUMAR, H.R. FOROOTAN, AND A. RASEKHI From the Transplant Research Center, Nemazee Hospital, Shiraz University of Medical Sciences, Shiraz, Iran. E.mail: geramib@sums.ac.ir.Telefax: 0711-6276211, P.O. Box: 71935-1119. Code Number: mr04005 ABSTRACT The aim of this study was to evaluate the role of fine needle aspiration cytology in the diagnosis of abdominal and retroperitoneal masses in children on this study. In 53 cases of childhood abdominal and retroperitoneal masses within a 4 year period (1998-2001) preoperative fine needle aspiration was done under the guide of CT scan. 2 pathologists reviewed fine needle aspiration smears. In all of the cases the gold standard for diagnosis was the tissue specimen, which showed 37 malignant, 2 benign neoplastic and 12 nonneoplastic diseases.This study showed that the sensitivity and specificity of fine needle aspiration cytology for the diagnosis of malignancy and benignity (positive or negative for malignancy) is 97.2% and 81.2% respectively. It was 100% accurate for the diagnosis of cell type in neuroblastoma-ganglioneuroblastoma, hepatoblastoma and Wilm's tumor, 77% accurate for lymphoma and 57% for germ cell tumors. There was no complication in any of the cases after fine needle aspiration. So fine needle aspiration is a reliable and sensitive method for the preoperative diagnosis of malignant pediatric abdominal and retroperitoneal masses and we recommend doing FNA cytology as a routine method for the diagnosis of such cases. Keywords: FNA, cytology, Abdominal, Retroperitoneal, masses, children. INTRODUCTION Preoperative diagnosis of abdominal and retroperitoneal masses in children is very important, because most patients with malignant tumors are treated with tumor specific chemotherapy regimens, so a pretreatment diagnosis is mandatory. The true nature of abdominal masses can be obtained only by microscopic examination of histologic or cytologic specimens and diagnosis by fine needle aspiration or tru-cut biopsy is an important approach.1 Fine needle aspiration cytology has been suggested as the method of choice for obtaining pretreatment diagnosis in childhood solid tumors1,2 but there are also reports that show some limitations in this era.3 The purpose of this study was to evaluate the diagnostic accuracy of fine needle aspiration cytology in abdominal and retroperitoneal tumors of childhood. MATERIAL AND METHODS To evaluate the role of fine needle aspiration in the diagnosis and differential diagnosis of abdominal, retroperitoneal and pelvic masses in children, 53 patients were selected during a 4-year period. In all of these 53 cases FNA was performed using a 22-23 gauge disposable needle under the guidance of CT scan by a radiologist. The smears were air-dried and alcohol-fixed and then stained by Wright and Papanicolaou stains respectively. Two pathologists without any knowledge about the final diagnosis reviewed all the cytologic smears. The pathologists didn't know anything about the history and imaging results of the patients. The only known data is an abdominal or retroperitoneal mass in a child. It is worthy to note that in all of these 53 cases a definite diagnosis was made by obtaining a tissue specimen after open surgery. All other cases in this 4 year period who were not operated and had no surgical specimen as a gold standard were omitted from the study population. RESULTSIn this study we had 53 cases including 32 boys and 21 girls in the age range of 3.5 months to 14 years (mean age 6 years). Among these 53 cases 12 cases were finally diagnosed as benign and nonneoplastic. As Table I shows 11 cases out of these 12 cases were correctly diagnosed by FNA as negative for malignancy. One of the cases that proved to be cirrhosis in the explanted liver after transplantation without any evidence of malignancy had been falsely diagnosed as malignant by FNA cytology. As Table II shows there were 4 cases with benign neoplastic tumors of which 2 were falsely diagnosed as malignant in FNA cytology. The remaining 37 cases were malignant tumors, including 4 cases of neuroblastoma, 1 ganglioneuroblastoma, 9 lymphomas, 7 germ cell tumors, 9 Wilm's tumors, 5 hepatoblastomas, 1 embryonal rhabdomyosarcoma and 1 metastatic osteosarcoma of the liver. Table III shows comparison of FNA cytology and final diagnosis in these 37 cases. In these 37 cases FNA cytology diagnosis was correct in 100% of neuroblastoma-ganglioneuroblastomas, hepatoblastomas, Wilm's tumors, 77% of lymphomas and 57% of germ cell tumors. The overall accuracy in diagnosis of malignancy in positive cases excluding benign cases was 86.5%. Table IV shows the overall accuracy of FNA cytology in 53 cases for diagnosis of the tumor as positive or negative for malignancy. As it is clear this study shows that the overall accuracy of FNA cytology for the diagnosis of benign and malignant abdominal and retroperitoneal tumors of children is 92.4%. It is worthy to note that we had a case of ganglioneuroblastoma which was diagnosed as neuroblastoma in FNA, but we considered it as a correct diagnosis. DISCUSSIONPreoperative diagnosis of abdominal and retroperitoneal masses of children is very important. Laparotomy for the sole purpose of establishing the diagnosis appears to be detrimental because of the possibility of perioperative morbidity and mortality.4 Diagnosis of abdominal and retroperitoneal masses by FNA may provide an alternative approach.4 In malignant tumors definitive cell typing is also necessary in order to institute the correct chemotherapeutic regimen.5 There are some reports in regard of the accuracy of FNA in abdominal masses of children in the last 10 years as below: In 1991 Edoute et al. reported 90% correct cell typing in 51 pediatric abdominal masses by FNA.5 This result was 94% by FNA and EM evaluation in a series of 62 cases in the study of Obers et al. in 1985.5 There are some reports with different results such as the study of Sabbah et al. in 15 cases. They concluded that FNA is either inconclusive or erroneous in 40% of cases and is an unreliable means for tumor typing.6 In one study in 40 cases of Burkitt's lymphoma, it was concluded that FNA is quite reliable.7 In the study of Miller et al. on 4 cases of neuroblastoma, FNA was found to be useful only in combination with immunohistochemistry, complete physical examination, radiology and laboratory tests.8 In another study by Quijauo FNA cytology was done in 10 cases of Wilm's tumor and found to be safe, with no complication and no evidence of dissemination attributable to the FNA procedure. They also concluded that FNA is a completely diagnostic procedure.9 In one study in 2 cases of hepatoblastoma, FNA was considered an accurate technique for the diagnosis of hepatoblastoma and proved to be a useful guide for surgeons and pediatric oncologists in therapy planning before surgery.10 In the study of Stanley et al. on 20 cases of germ cell tumor, FNA proved to be highly accurate and 19 of the 20 cases were diagnosed correctly.11 In our study in nonneoplastic masses only one case was diagnosed incorrectly as malignant and all other 11 cases were accurately diagnosed as nonneoplastic. In 4 benign neoplastic specimens 2 cases were false positive including one inflammatory pseudotumor which was diagnosed as lymphoma and the other one which was a case of ovarian papillary cystadenoma which was diagnosed as small round blue cell tumor. Among 37 malignant cases, 36 cases were correctly diagnosed as malignant but diagnosis of the type of tumor was correct in all 5 cases of neuroblastomaganglioneuroblastoma, 9 Wilm's tumor and 5 hepatoblastoma. In 9 cases of lymphoma the correct cell typing was done in 7 patients. We had 7 germ cell tumors, of which diagnosis of the tumor type was correct by FNA in 4 of them. According to the above results, our study indicates that FNA cytology is a sensitive mean for diagnosis and cell typing of most common malignant intraabdominal tumors of children. The sensitivity and specificity of FNA cytology in 53 cases were 97.2% and 81.2% respectively for the diagnosis of a lesion as benign or malignant and its accuracy for diagnosis of the tumor type of malignant ones was 86.5%. We had a case of ganglioneuroblastoma which was diagnosed as neuroblastoma by FNA, therefore, in neuroblastoma, ganglioneuroblastoma should always be considered especially if large cells with large, vesicular nuclei and prominent or multiple nucleoli are frequent. In FNA smears of liver, metastasis should always be considered. We had 2 liver metastases, one from osteogenic sarcoma and the other was a case of immature teratoma. Therefore clinical history has paramount importance in these cases. The other important point in liver masses is cirrhosis and granulomatous inflammation. So these two need to be in mind in the evaluation of any liver FNA smears. Overall in benign neoplastic lesions FNA should be supported by clinical history, physical examination and imaging techniques to be more accurate.Finally according to the present study we think that FNA cytology under the guidance of CT scan or sonography interpreted by an experienced cytopathologist is a very effective method for diagnosis and cell typing of abdominal and retroperitoneal masses in children. REFERENCES
Copyright 2004 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr04005t2.jpg] [mr04005t3.jpg] [mr04005t4.jpg] [mr04005t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}