 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
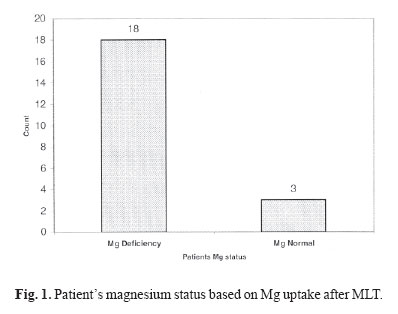
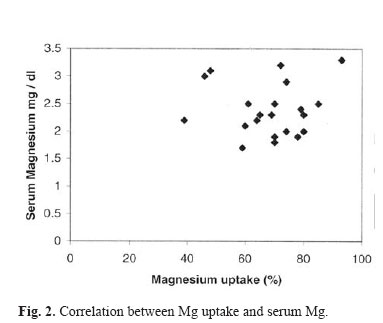
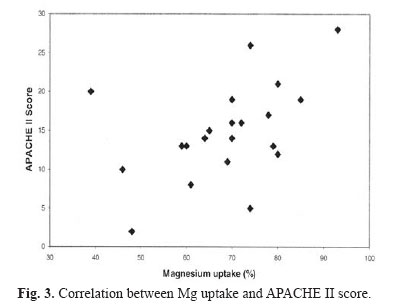
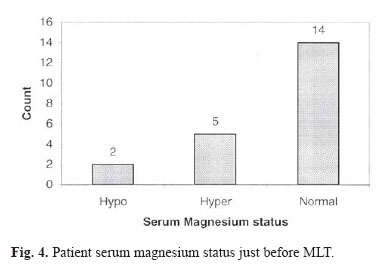
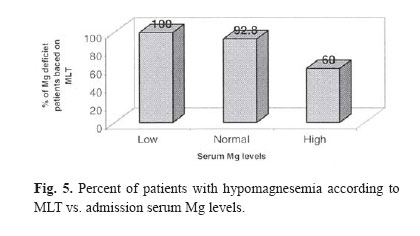
Medical Journal of the Islamic Republic of Iran , Vol. 18, No. 1, May, 2004, pp. 35-38 ROLE OF MAGNESIUM LOADING TEST IN DETECTING HYPOMAGNESEMIA IN CRITICALLY ILL PATIENTS S.M. SOHREVARDI,* M. MOJTAHEDZADEH,** S. SADRAY,*** A. NAJAFI,** J.D. SPENCE,**** C. MUNOZ,**** AND H. TAVAKOLI** From the *Faculty of Pharmacy, Kerman University of Medical Sciences, Kerman, I.R. Iran, **Intensive Care Unit, Sina Medical Center, Tehran University of Medical Sciences, the ***Faculty of Pharmacy, Tehran University of Medical Sciences, Tehran, I.R. Iran, and the ****Stroke Prevention and Atherosclerosis Research Centre, LHSC, Canada. Code Number: mr04006 ABSTRACTMagnesium (Mg) deficiency has not usually been considered in clinical practice due to lack of relevant blood tests and because the symptoms are often vague and nonspecific. Serum concentrations may not adequately reflect Mg status. Mg Loading Test (MLT) can provide information on total body Mg stores. We prospectively studied 21 critically ill patients (10 male,11 female) admitted to the ICU, to investigate the prevalence of Mg deficiency. Their mean age was 50±21 years. To determine serum Mg, venous blood specimens were obtained just before the MLT. Mg sulfate (30 mmol) was infused during an 8-hr period and 24-hr urine samples were collected from the starting of Mg infusion. Although low serum Mg (< 1.8 mmol/L) was present only in 2 patients, MLT showed Mg deficiency in 18 patients. MLT detected Mg deficiency in 13 out of 14 patients with normal serum Mg, in 2 out of 2 subjects with hypomagnesemia, and in 3 out of 5 cases with hypermagnesemia. Of 7 fetal cases, 6 oc curred in individuals with hypomagnesemia (6/18) and 1 death occurred in the normomagnesemic group (1/3). There was no relationship between Mg retention, age (r= 0.33, p= 0.63) and serum Mg concentrations (r= 0.15, p= 0.925). There was a significant correlation between Mg uptake and APACHE II score (r= 0.46, p= 0.035). In conclusion, Mg depletion is highly prevalent in ICU patients according to MLT. MLT is superior to serum Mg in determining actual Mg status in this group. Therefore, we suggest that MLT, and not serum Mg, should be carried out in patients when Mg deficiency is suspected. Keywords: Magnesium Loading Test, Serum magnesium, Intensive Care Unit, APACHE II Score. INTRODUCTION Magnesium (Mg) is the fourth most abundant cation in the body and the second most prevalent intracellular cation. Mg is primarily located in bone (65%) and muscle (20%). Total body store is approximately 21-28 g. It serves as a cofactor for about 300 cellular enzymes.1,2 Magnesium is essential for virtually all hormonal reactions that occur in the body.3 It plays an essential role in the function of the cell membrane sodium-potassium ATPase pump.4 Mg is a calcium channel blocker.5 Hypomagnesemia may cause symptoms and signs of disordered function of the cardiac, neuromuscular and central nervous system. It is also associated with imbalance of other electrolytes, such as K+ and Ca2+ .6 Hypomagnesemia may result from gastrointestinal or renal losses, from cellular redistribution of Mg7 or from malnutrition.8 Since only 1% of total body Mg is in the extracellular fluid, serum Mg concentrations may not adequately reflect Mg status. Significant Mg deficiency may exist while plasma Mg concentration is normal. Thus, normal serum Mg could constitute a serious underestimation of the severity of Mg defi-7,9,10 Among three Mg fractions in serum (protein bond, ionized and ultrafiltrable fraction) only the ionized fraction is physiologically active. However the simplest and possibly the most reliable test used in the assessment of functional magnesium deficiency is believed to be the Magnesium Loading Test (MLT). MLT is feasible and appears to be valid and provide substantial information on total body Mg stores in critically ill patients. Using the MLT as a reference, both serum total and ionized Mg assays are insensitive biochemical markers of functional hypomagnesemia.11 The serum Mg concentration, though an insensitive measure of Mg deficit, remains the only practical test of Mg status in widespread use. Surveys of serum Mg levels in hospitalized patients indicate a high incidence of hypomagnesemia (presumably an underestimate of the true incidence of Mg deficiency), ranging from 11% to 47% in general patients12,13,14 and 20% to 65% in patients admitted to intensive care units.14,15,16 This study was conducted to estimate the prevalence of Mg deficiency in ICU patients at Sina hospital (Tehran-Iran). MATERIAL AND METHODSThis study was a cross-sectional survey on 21 cases who were admitted for at least 48hrs in our intensive care unit (ICU). The study was approved by the investigational review board of Tehran University of Medical Sciences. The exclusion criteria were impaired renal function (serum creatinine > 1.5mg/dL) and known cases of renal failure, heart rate<60 beats/min, severe metabolic disturbances, diuretic therapy, coagulopathy, magnesium supplements, myasthenia gravis or any other known neuromuscular diseases. The MLT was performed as described in detail earlier.17 30mmole (7.5g) of Mg sulfate was administered as a continuous intravenous infusion for an 8hr period.11,19 Mean arterial blood pressure, electrocardiogram, pulse rate, respiratory rate and deep tendon reflexes were recorded to detect any sign of hypermagnesemia. Urine samples were collected in plastic bottles acidified with 15 mL 10% HCl from the start of the infusion for 24hrs.20 The uptake of Mg was calculated from the Mg dose given intravenously and the amount excreted during the study time and expressed in percent of the amount of Mg given. (30mmol Mg2+ Infused - Amount of Mg2+ excreted in urine)*100 / (30mmol Mg2+ infused).1,17 The Technicon RA-XT was used to analyse urine and serum Mg content. Venous blood specimens were obtained before MgSO4 administration. Magnesium deficiency was defined as <50% Mg excretion over a 24hr period.18 Statistical analysis was performed using Chi-square for categorical variables, and Pearson Correlation coefficient was used to correlate data with normal distribution. RESULTSMean patients age was 50±21years (10 male, 11 female). Magnesium uptake (retention) in patients ranged from 39 to 93% with a mean value of 68.4% ± 13.2 . Based on MLT, 18 patients had definite Mg deficiency and only 3 patients were normal (Fig. 1). The Pearson correlation coefficient ( r ) showed no linear relationship between Mg retention, age (r=0.33, p=0.63) and serum Mg (r=0.15, p=0.925). Fig. 2 shows the correlation between Mg retention and serum magnesium. There was no correlation between Mg uptake and sex (Chi2 =14.3,P=0.575). However, there was a positive correlation between Mg uptake and patient's disease severity as defined by their APACHE-II score21 (r=0.46, p=0.035) (Fig. 3). APACHE II uses a point score based upon initial values of 12 routine physiologic measurements, age, and previous health status to provide a general measure of severity of disease. An increasing score (range 0 to 71) was closely correlated with the subsequent risk of hospital death.21 Serum Mg concentrations (just before MLT) were higher in 5 patients, lower in 2 patients, and normal in 14 patients (Fig. 4). Mg deficiency (according to MLT) was interestingly detected in 13 patients whose serum Mg were normal, in all hypomagnesemic cases and in 3 hypermagnesemic ones (Fig. 5). Finally 7 patients out of 21 died and there was no difference between normomagnesemic and hypomagnesemic (according to MLT) groups. DISCUSSIONThis study shows the importance of MLT in determining the true Mg status in ICU admitted patients. In agreement with previous studies,19 Mg deficiency was highly prevalent in critically ill patients. MLT was able to detect Mg deficiency in 18 out of 21 critically ill patients whereas serum Mg levels indicated deficiency only in 2 of those patients. As the MLT appears to better reflect the true Mg status of patients, it should be the test of choice when assessing for Mg deficiency. Mg deficiency seems to be more common in our study population than others. According to our definition of Mg deficiency (<50% Mg excretion in 24hr urine from 30mmol Mg given in MLT) Mg deficiency was present in 85.7% of critically ill patients, whereas the frequency reported by others,11,14,15,16 using the same definition and also in ICU admitted patients, was 20-65%. According to the definition for Mg deficiency used by other au-11,17,19 (<70% Mg excretion of the total Mg given) all subjects in our study could be considered Mg deficient. This study confirms that serum magnesium is not a reliable method to determine the magnesium status in critically ill patients. Hebert et al.11 noted that only 2 patients had low total serum Mg in a group of 12 cases with Mg deficiency according to MLT. Similarly, in our study, only 2 critically ill patients had low total serum Mg out of 18 cases with Mg deficiency as diagnosed by MLT. In addition, there was no correlation between total serum Mg concentration and Mg retention during MLT. This disparity between serum Mg concentrations and MLT is explained by the fact that 99% of Mg is found in the intracellular compartment making it difficult for serum assays to the reflect functional Mg status.11 This is in agreement with reports indicating a lack of association between Mg serum levels and clinical outcomes. For example, Rubeiz et al.14 showed that hypomagnesemic and normomagnesemic groups had comparable APACHE II scores and other clinical variables except for mortality. Mortality rates of hypomagnesemic patients were approximately twice (p<0.01) the rate of the normomagnesemic group. In addition, the duration of hospital survival in those patients who died was approximately 8 days less for hypomagnesemic than normomagnesemic patients. Unfortunately, MLT was not performed in that study. We predict that mortality would be even greater in Mg deficient than non-deficient individuals. In our study, there was a significant correlation between Mg uptake during MLT, and APACHE II score (r=0.46, p=0.035). The proportion of fatal cases were similar in deficient (6/18) and non-deficient (1/3) patients, in part because we corrected Mg deficiency upon diagnosis. Magnesium has been implicated in the physiopathology of clinical conditions often found in critically ill patients such as cardiac arrhythmias, congestive heart failure and significant impairment of neurological functioning. Thus, identification and correction of Mg deficiency is very important. Because Mg deficiency may exist while plasma Mg concentration is normal,7,9,10 serum magnesium concentrations may not accurately reflect total magnesium stores in all compartments.23,24 On the basis of these results, we concluded that MLT should be carried out in patients in whom Mg deficiency is suspected, particularly, in cases with normal or increased serum magnesium. REFERENCES
Copyright 2004 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr04006f5.jpg] [mr04006f4.jpg] [mr04006f3.jpg] [mr04006f1.jpg] [mr04006f2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}