 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Medical Journal of the Islamic Republic of Iran , Vol. 18, No. 1, May, 2004, pp. 39-43 PREVALENCE OF CELIAC DISEASE IN CHILDREN AND ADOLESCENTS WITH TYPE I DIABETES MELLITUS H. MOAYERI AND S.H. BAHREMANDFrom the Pediatrics Department, Imam Khomeini Hospital, Faculty of Medicine, Tehran University of Medical Sciences, Tehran, Iran. Correspondence: H.Moayeri, Department of Pediatric Endocrinology, Imam Khomeini Hospital, Faculty of Medicine, Tehran University of Medical Sciences, Tehran, Iran. Tel: + 98218004446, Fax: + 98218270902, E. Mail: H. Moayeri @ radsa net. Code Number: mr04007 ABSTRACTThe association of celiac disease and type I diabetes mellitus has been known for some time. This study was undertaken to investigate the prevalence of celiac disease (CD) in diabetic children and adolescents. Eighty-seven patients (44 females, 43 males) aged 2- 18 years, with type I diabetes participated in this study. A group of 87 healthy unrelated girls and boys matched for age and gender served as controls. They were screened for the presence of celiac disease related marker [IgA - endomysial antibody (EMA)] and patients who were EMA positive further investigated with intestinal biopsy. Among diabetic patients a 3.4% prevalence of celiac disease was observed, a value significantly higher than that found among healthy controls. Girls were more frequently EMA positive than boys. Intestinal biopsies of all 3 patients with positive EMA showed a histologic picture confirming the diagnosis of CD. Diabetics with CD were significantly younger, had an earlier onset of diabetes, had a lower height and weight standard deviation score and poorer glycemic control compared with diabetics without CD (p<0.05). We failed to show any significant correlation between EMA- positivity and duration of diabetes. The results suggest EMA - positivity to be a good immunological marker for use in screening for celiac disease and such screening to be justified in our patients with type I diabetes mellitus, regardless of diabetes duration. Keywords: Adolescents, Children, Celiac disease (CD), IgA - endomysial antibody (EMA), Type I diabetes mellitus. INTRODUCTION Type I or insulin dependent diabetes mellitus (IDDM)
is an organ–specific autoimmune disease in which T-cell
mediated destruction of pancreatic beta cells take place.
Gluten-sensitive enteropathy or celiac disease (CD) is a
heterogeneous disorder involving abnormalities in the
small intestinal mucosa (villous atrophy and crypt hyperplasia),
which ranges from silent asymptomatic forms
to active malabsorption syndromes.1,2 Although the pathogenesis of the disease remains unclear, it involves
genetic determinants and environmental factors together.
Gluten has been identified as the trigger molecule in CD
development. The presence of different antibodies
(antigliadin, antiendomysial, antireticulin and others) are
indicative of possible CD, but diagnostic confirmation
is based on histologic examination of specimens obtained
in intestinal biopsy. The association of type I diabetes
mellitus and CD has been known for some years3-10 and
in initial studies based on clinical data, a prevalence of
approximately 1% to 1.5% has been calculated among
patients with diabetes. However, within the past few
years several studies have shown the prevalence of CD
in diabetes to be even higher than considered previously.
The use of CD–specific immunologic markers in
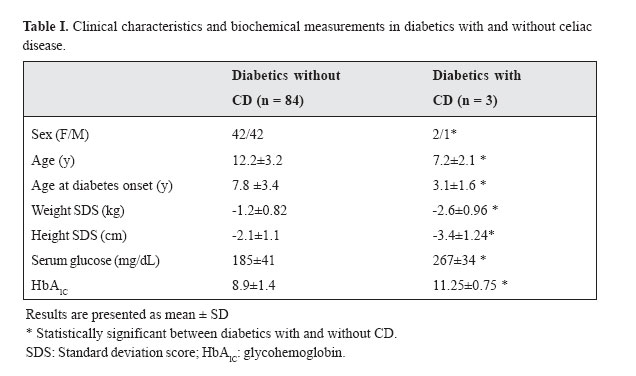
MATERIAL AND METHODS Subjects Eighty - seven patients (44F, 43M) with type I diabetes mellitus (median diabetes duration 4.1 years, range 1-12 years) were studied at the Pediatrics Department of Tehran University of Medical Sciences. The age range of the study participants was 2-18 years with a mean age of 11.7 ± 4.5 years. They were diagnosed as having diabetes type I on the basis of World Health Organization (WHO) criteria.27 The patients initially showed typical symptoms of hyperglycemia and 48.9% of them presented with ketoacidosis or impaired consciousness as the first manifestation of the disease. All of the patients required insulin replacement therapy for survival or to achieve adequate metabolic control from the time of diagnosis. ControlsControl subjects included 87 age and gender matched normal children (43F, 45M) with a median age of 11.1±3.9 years, range 3-18.5 years. None of the control subjects disclosed any symptoms compatible with CD and none were growth retarded. None of them had a family history of type I diabetes or CD. Age, sex, age at onset of diabetes, daily dose of insulin injection, weight and height were recorded in a questionnaire. Each patient and control were requested to fill a questionnaire by answering yes or no to a set of questions regarding symptoms of CD. MethodsAfter ruling out IgA deficiency in all subjects IgA class endomysial antibody (EMA) was measured by an immunofluorescence technique as an initial screening test for CD. In diabetic patients, serum glucose concentration and glycohemoglobin (HbA1c) were measured. Intestinal biopsySubjects with EMA were offered intestinal biopsy. Endoscopic duodenal biopsies were taken and examined histologically by an expert pathologist. Diagnosis of celiac diseaseCD was diagnosed when the intestinal mucosa showed partial or total atrophy, crypt hyperplasia and intraepithelial lymphocytic infiltration according to the latest criteria of the European Society for Pediatric Gastroenterology Hepatology and Nutrition (ESPGHAN).28 Statistical analysisAll results are presented as the mean±SD. Comparison between groups was performed using Student's t-test. A p value of 5% or less was considered statistically significant. RESULTSAmong the 87 patients with type I diabetes, 3 (3.4%) were positive for EMA. In the control group none had EMA. None of the subjects and controls were IgA deficient. Three EMA positive patients exhibited histologic findings in their intestinal biopsy specimens supporting the diagnosis of CD. The diabetics with CD did not report any symptoms indicating CD at the first interview. At the time of biopsy, about 6 months later two patients showed symptoms compatible with CD (loose stools, abdominal discomfort). Clinical characteristics and biochemical measurements in diabetics with CD and without CD are compared in Table I. The diabetic patients with CD had a median age of 7.2 ± 2.1 yr at the time of screening and a median duration of diabetes of 3.5 ± 1.8 yr compared with 12.2 ± 3.2 yr and 4.1 ± 1.7 yr respectively in diabetics without CD. The diabetic subjects with CD were significantly younger than the group of diabetics without CD. They also had an earlier onset of diabetes, mean age 3.1±1.6 yr compared with 7.8 ± 3.4 yr in patients without CD (p<0.05). In diabetic patients with CD the mean height standard deviation score (SDS) was -3.4 ± 1.24 cm compared with -2.1 ± 1.1 cm in patients without CD. In patients with CD, the mean weight SDS was - 2.6 ± 0.96 kg compared with -1.2 ± 0.82 kg in patients without CD. So in patients with CD the mean height and weight SDS were significantly lower compared with diabetes without CD. There were significant differences between the two groups with regard to the glycemic control (the mean glucose concentration was 267 ± 34 mg/ dL vs 185 ± 41mg/dL; HbAIc : 11.25 ± 0.75 vs 8.9 ± 1.4 percent in patients with CD and without CD respectively). DISCUSSIONThe prevalence of CD among diabetic patients ranges from 0.61% to 7.8% in various reports3-10 but recent studies based on screening results with the sensitive EMA method show the highest prevalence of CD to be between 2.8% and 16.4%.11-17 In the present study, out of 87 children with type I diabetes, 3 patients met the revised ESPGHAN criteria for celiac disease,28 resulting in a prevalence of 3.4% of CD among diabetic patients in our study group. The differences among results in various studies may be because of the difficulty of accurately evaluating the frequency when estimated from clinical findings and many initial studies were based on this method. Patients in risk groups such as diabetics represent a special case, as they may be symptom-free. So the existence of subclinical forms of the disease (silent or latent CD) that may not be accounted for, and the different antibody detection methods [antigliadin antibody (AGA)] as initial screening tests29-31 could explain this discrepancy. Because as previously reported21, 26, 32-34 AGA was not reliable, only a small proportion of isolated AGA positive patients exhibit pathologic mucosa. Finally, the wide range of prevalences in various reports may also be due to differences in ethnic groups, geographic area and population size in each report. In the present study, CD was more frequent in female patients, and diabetics with CD had a significantly earlier onset of diabetes, had a lower height and weight SDS and poorer glycemic control compared with diabetics without CD (p<0.05). Diabetic patients with CD were significantly younger than the group of diabetics without CD, possibly indicating that patients have a more aggressive autoimmune disease response. We failed to show any significant correlation between CD and diabetes duration, similar to the majority of previous reports.11,14,15,16 In the present survey and other studies14-17 all EMA positive patients who underwent intestinal biopsy had CD, thus showing the predictive value of EMA positivity to be as high among patients with type I diabetes as the general population. In summary, EMA analysis is considered to be the most powerful tool currently available for serologic screening of CD at least in children above 2 years of age.35-36 Some authors suggest regular screening with CD related antibodies in children with type I diabetes.13,37 In Iran routine screening for CD disease related antibodies in diabetics is not common practice. Thus, from a clinical point of view, EMA screening should be a part of health assessment in patients with type I diabetes, because diabetic patients with CD diagnosed by screening often have no or only mild symptoms of the disease. However, a gluten-free diet in asymptomatic patients may not only increase the general well - being of the patients and improve glycemic control but also prevent the well - known complications of CD, such as malnutrition, growth failure, pubertal delay, osteoporosis, infertility and intestinal malignancies.38-40 REFERENCES
Copyright 2004 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr04007t1.jpg] |
| |||||||||
{kind=link}