 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
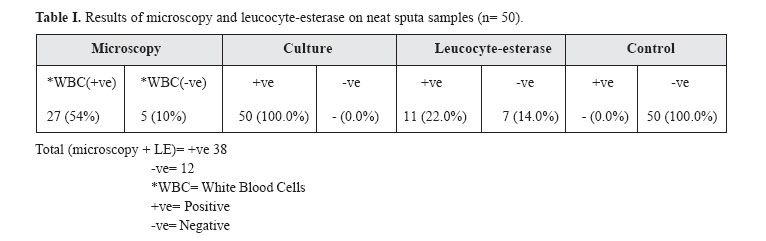
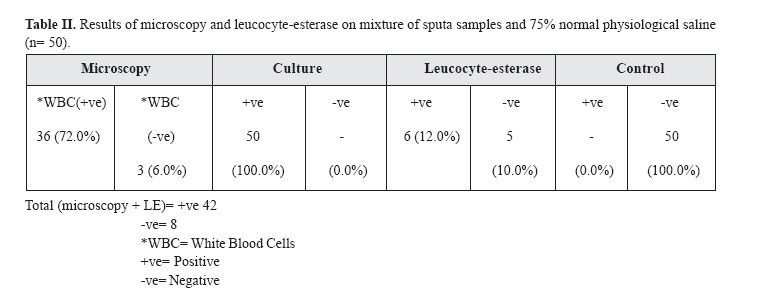
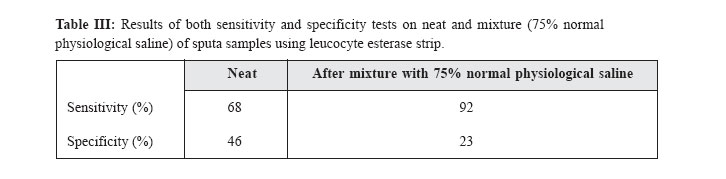
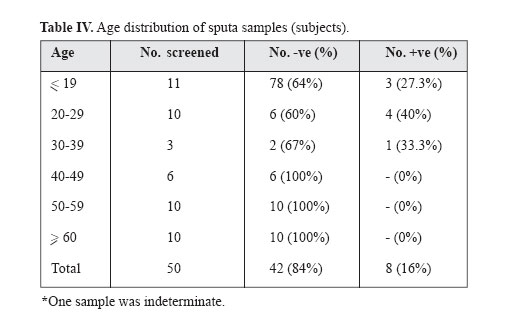
Medical Journal of the Islamic Republic of Iran , Vol. 18, No. 1, May, 2004, pp. 67-71 USE OF LEUCOCYTE-ESTERASE AS A MEANS OF TESTING SUITABILITY OF SPUTUM SPECIMENS FOR LABORATORY EXAMINATION N.C.D. UKWANDU*,1 J.O. CHIKWEM,1 A.E. MOSES,1 M. JAJUA,1 C.O. ELEMUWA,2 J. OKPE3 AND S. IWUANYANWU3 From the 1Department of Medical Microbiology, College of Medical Sciences, University of Maiduguri, P.M.B. 1069, Maiduguri, Nigeria, the 2Central Public Health Laboratories, Yaba, Lagos, Nigeria, and the 3Department of Medical Microbiology, University of Lagos Teaching Hospital, Idi-Araba, Lagos, Nigeria. *Correspondence and Present Address: Department of Medical Microbiology, Faculty of Clinical Sciences, College of Medicine, Edo State (Ambrose Ali) University, P.M.B. 14, Ekpoma, Nigeria. Code Number: mr04011 ABSTRACTThe study has strived to compare the leucocyte-esterase stripe activity on sputum samples with gram-stained direct smear microscopy. This is for the demonstration of white blood cells (WBCs) and so to develop a simple method for selecting suitable sputum samples for cultural examination and laboratory diagnosis. A total of 17(34.0%) out of 50 samples studied were shown to be unsuitable for microbiological examination and for identification of mycobacterial infection. Sputa of patients between the ages of 20-29 years old were found to be more positive by demonstrating more WBCs and squamous epithelial cells (SECs). We believe this technique should offer an alternative to the conventional direct smear microscopy used for examining patient's sputa in our hospital laboratories. Keywords: Sputum, Leucocyte-esterase, laboratory. INTRODUCTIONThe morbidity and mortality due to tuberculosis in both the developed and developing nations of the world have given a great concern especially with the concurrent human immunodeficiency virus infection (HIV).1,2,3 Dolin et al.4 have estimated a total of about eighty-eight million people with tuberculosis world-wide over a period of 10 years before the end of the 20th century, with a total of about thirty million people expected to die. The great concern which this infection has posed is enormous in developing nations such as in Africa where about 80% of the infection is concentrated.5,6 This concern is worsened by the non-availability of adequate laboratory infrastructures for examination and diagnosis of laboratory sputa samples.3,7 The provision of automatic results is a function of qualitative samples in any microbiology laboratory.3 Chikwem et al.3 have suggested the need to devise more sensitive techniques for diagnosing mycobacterial infection so as to control the spread of mycobacterium among susceptible individuals as well as ensure early treatment of those already infected. The production of sputa could be associated with diagnostic problems due to the presence of normal flora in the upper respiratory tract. This flora contains pathogens which are potentially associated with diseases of the lower respiratory tract. The reported high prevalence of HIV infections in some developing nations has further worsened the problem of tuberculosis.8 Murray9 and Chikwem et al.3 have highlighted methods which can be used to microscopically access samples from the respiratory tract, while Laired10 has enumerated criteria on which each of these methods should be based. Daley11 believed that squamous epithelial cells and white blood cells are characteristics of the secretion from oropharyngeal and lower respiratory tract regions of the body anatomy respectively. Because of the probability of the contamination of the oropharyngeal region,12 it has been accepted in practice that sputa samples which have less than ten white blood cells per low power field (<10 WBC/Lpf) and more than twenty-five squamous epithelial cells per low power field (>25 SEC/Lpf) are taken to be unsuitable for laboratory examination and diagnosis. In the microbiology laboratories, Chikwem et al.3 showed that both the presence of infective organisms and/or contamination are confirmed by one of the methods e.g. gram-staining of the smear after processing samples and examining the slide microscopically. The authors established that the gram stain technique has flaws and these are: requirement of a lot of effort, technical skill, and it is time consuming. Besides, the reward from this technique is minimal. The reported high prevalence of HIV infection in some of these developing nations has further bedeviled the problems of tuberculosis diagnosis.8 There is urgent need therefore, to intensify the National Control Programmes on Tuberculosis in some developing nations of the world. The presence of significant WBCs (>10 WBC/ Lpf) indicates an inflammatory response while the isolation of potential pathogens is doubtful in the absence of WBC especially in immunological responsive individuals. It goes without doubt to accept that if sputa can be screened for the presence of significant WBC, and rejecting those sputa without significant WBC, as being unsuitable for microbiological examination, much time and effort would have been saved. This could increase the level of confidence in the significance of any isolates in the sample. We therefore decided to investigate the suitability of sputa samples for culture by using leucocyte-esterase. This was done by comparing results of leucocyte-esterase (LE) test procedure, and the gram-stain smears examined under light microscopy as routine screening method of sputa samples for culture. MATERIAL AND METHODSFifty sputum samples from fifty clinically confirmed tuberculosis (TB) patients were screened using the leu-cocyte-esterase strip test procedure of multistix and SG reagent strips from Bayer Diagnostics.13 The patients belonged to all age groups and comprised thirty-two males and eighteen females. They were further confirmed positive for TB by cultural method after clinical and physical observations. The principle behind the mechanism of action of leucocyte-esterase (LE) is that it liberates indoxyl on insertion into sputa samples, from the indoxyl carbonic acid substrate incorporated in the strip.13 LE action was tested on the sputum specimen by insertion of the esterase area of the strip into the sputum. The colour change thereafter was compared with the interpretation colour chart on the side of the strip container. The sputa were tested twice. First, they were tested directly and secondly, after mixing volume by volume with normal 75% physiological saline. Sputa smears were made on greaseless microscope slides before mixing and air-dried. These smears were stained using gram's method,14 and examined under ×10 magnification using a light microscope for the presence of white blood cells. Information regarding the biodata and previous background of each of the patients were obtained after collecting these from them as they submitted their sputa specimens. Controls were comprised of 10 sputa samples from apparently healthy individuals. RESULTSTable I shows the result of microscopy and LE activity on neat sputa samples. A total of 11 sputa were positive while 7 (14.0%) were negative for LE. The results of the microscopy shows 27 (54.0%) and 5 (10.0%) sputa samples to be positive and negative respectively. The cultural method confirmed the 50 (100.0%) sputa samples positive. The total sputa samples confirmed positive by microscopy and LE were 38 (76.0%) while 12 (24.0%) were negative. Table II shows the results of microscopy and LE activity on mixed sputa samples. LE activity detected 6 (12.0%) positives and 5 (10.0%) negatives from the 50 sputa samples. Six of the LE positive sputa samples had >25 SEC/Lpf, and thus gave a total of 17 (34.0%) sputa samples that were regarded as unsuitable for cultural examination. The total sputa confirmed positive by microscopy and LE were 42 (84.0%) while 8 (16.0%) were negative. Table III shows the results of sensitivity and specificity of LE activity on both neat and homogenized sputa samples. The sensitivity of the LE was higher for the homogenized sputa (92.0%) while its specificity was higher (46.0%) for the neat sputa. Table IV shows the distribution of the sputa samples amongst the various age groups screened. The peak positivity rates fell between the age groups of 30-60 years old. DISCUSSIONThere have been reports from workers like Chikwem et al.3 and Geckler et al.15 who have compared the different methods of detecing mycobacterial infections from sputum. Also, Geckler et al.15 have compared results from cultures of sputum and transtracheal aspirates from the same patients. Their results concluded that cultural methods (30.0%) were more sensitive than the other two methods. These two methods were concentrated smear technique (26.0%) and direct technique (15.0%). However, their work lacked the cognizance of the quality of the sputa samples used. Gecker et al.15 found 79.0% agreement between culture results of two sputa specimens when sputum had <25 SEC/Lpf at ×100 magnification and 27.0% agreement when sputum had >25 SEC/Lpf. What this means is that notwithstanding the quality of sputa, cultural method proved better than the other two commonly known methods. The workers also found that 36.0% of contaminated sputa samples contained potential pathogens which were not present in the corresponding aspirates. Kumararatne et al.16 therefore suggested that, it then becomes obvious that the principal indicator in determining whether there is contamination of sputum specimen from the oropharyngeal region is the presence of SEC in samples, while the presence of WBC indicates inflammatory reactions, notwithstanding the numerical counts. If the presence of WBC is suggestive of inflammatory activity, the isolation of potential pathogens in their absence from immunoresponsive individuals, or even in the absence of SEC becomes difficult to explain. However, the only rational explanation would be that the pathogens are effective, or endogenous and not reticular and therefore have gone through the major histocompatibility complex-1 (MHC-1) pathway. This study never went into determining the different antibody levels. Similarly, LE-test showed a better sensitivity than direct smear microscopy in detecting WBC in sputa samples. The apparent lack of good specificity of LE-tests after mixing the sputa with 75.0% normal physiological saline, could be due to the lack of sensitivity of microscopy when low. WBC counts suffice. This could also be worse when there are cell's lyses. Glaister17 has said that as an indicator of contamination, the microscopy of a gram-stained smear is good, but as a predictor of result from culture, it is not encouraging. Therefore, being most useful for predicting negative results, it can then be proposed that, LE-test provides a simple alternative to the gram film for the screening of sputum specimens. Sputa should be rejected if the LE-test is negative. If LE-test is positive, then gram-film should be done to quantify SEC. Sputa specimens with >25 SEC/Lpf should be rejected if there is a 36.0% chance of isolating a pathogen17 of dubious and fake significant identity from samples. If it becomes increasingly difficult to obtain a good sample, it is wise to obtain samples by the invasive method. This, however, is possible when patients are few. The high prevalence of WBC and SEC, amongst individuals within the age bracket of 30 years and above, can be associated with the dynamism of interactions and other sociocultural behaviours associated with this group. These predispose individuals to infections and diseases. Using Leucocyte-esterase strip, 11(22.0%) of the homogenized specimens were LE-negative. Six more samples from the LE-positive group had >25 SEC/Lpf thus giving a total of 17(34.0%) samples which were unsuitable for microbiological and bacteriological examination. These Figures were quite high when compared with the results of Hugh and Newall.12 These two workers had in their recent work, reported of 14(7.0%) LE-negatives from homogenized samples and 22(11.0%) specimens considered to be unsuitable sputa. This was very low when compared with the results of Abbas et al.18 They also reported 22.0% of the homogenized specimens to be LE-negative while 8.0% of the LE-positive specimens showed evidence of oropharyngeal contamination. It can be said that those specimen samples which were rejected because they were LE-negative will allow for a concentration of resources on positive specimens and foster high confidence in results which will be gotten from them. ACKNOWLEDGEMENTSThe authors are grateful to the patients who provided the sputa samples and also to the management of University of Lagos Teaching Hospital (LUTH), Central Public Health Laboratory, and University of Maiduguri Teaching Hospital (UMTH) for laboratory facilities. We are also grateful to Mr. Bona Nlemadim, Director of Borno Central Medical Laboratory and Mr. Chris Elemuwa for the provision of laboratory space and leucocyte-esterase strips respectively. REFERENCES
Copyright 2004 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr04011t1.jpg] [mr04011t3.jpg] [mr04011t4.jpg] [mr04011t2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}