 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Medical Journal of the Islamic Republic of Iran , Vol. 18, No. 2, August, 2004, pp.107-110 CORRECTED QT DISPERSION IN CHILDREN WITH ISOLATED UNCOMPLICATED MITRAL VALVE PROLAPSE ELAHEH MALAKAN RAD, AND NADER MOMTAZMANESH From the Department of Pediatrics, Kashan University of Medical Sciences, Kashan, I.R. Iran. Address: Kashan University of Medical Sciences, Ghotb Ravandi Blvd., Kashan 87154, I.R. Iran. Tel: (0361)-552999-8268752 Fax: (0361)-552999, malakan_rad@Kaums.ac.ir Code Number: mr04019 Mitral valve prolapse (MVP) is a relatively frequent valvular abnormality. In both children and adults with MVP, an increased incidence of ventricular arrhythmias has been reported. QT dispersion, defined as the difference in duration between the longest QT interval and the shortest one, for a given set of electrocardiographic leads has been proposed as a sign of regional difference in cardiac repolarization and as a marker of increased risk of ventricular arrhythmias. This study was designed to compare the corrected QT dispersion (QTcD) in children with isolated uncomplicated prolapse with a normal age-and sex-matched group of children. Twenty children with MVP (mean+SD age: 8+5 years) and thirty normal children enrolled in the study. Corrected QT dispersion was manually calculated on their surface electrocardiogram in all of them. QTcD was 39+14.7 and 40+15.2 milliseconds respectively. An unpaired Student t-test was performed. There was no significant difference between! the mean value of the two groups (p value<0.01). The findings of our study, besides the reports of increased QT dispersion in adults, suggest that increased QT dispersion in patients with MVP is a time-evolved phenomenon and does not exist from the very early years of age. Keywords: Corrected QT dispersion, Mitral valve prolapse, Children. INTRODUCTION Ventricular arrhythmias are seen in patients with mitral valve prolapse (MVP) with increased frequency.1-2 The contribution of this heterogeneity of the repolarization process within the myocardium for triggering ventricular arrhythmias has also been already recognized.3,4,5 The existence of an abnormal pattern of ventricular repolarization has been exclusively demonstrated.6-7 Corrected QT dispersion (QTcD), measured in the 12- lead surface electrocardiogram is a simple approach to the evaluation of ventricular repolarization.8 Despite relatively extensive research on QT dispersion in adults with mitral valve prolapse,9-15 to our knowledge no or perhaps few studies have addressed the issue of QT dispersion in children with MVP. The aim of this study is to determine whether QT dispersion of children with MVP is different from normal controls. MATERIAL AND METHODS A resting 12-lead electrocardiogram was obtained
from 20 children with uncomplicated isolated MVP, including
12 females and 8 males (aged 3 to 14 years,mean
[±SD]age:8±5 years). Only children who had both the
echocardiographic and auscultatory findings of MVP
were included.On echocardiography, mitral valve prolapse
was diagnosed only when there was definite prolapse
of the leaflets observed in at least two
echocardiographic planes (parasternal long-axis and four
chamber views).16 None of our patients had MR, either
on auscultation or echocardiography. Prolapse was defined
as displacement of one or both mitral leaflets by more than 2 millimeters above the high points of the mitral annulus. Individuals who were on drug therapy that could potentially affect QT characteristics were excluded. Thirty age- and sex-matched healthy children were enrolled in the study as control. Children who were referred for the evaluation of a cardiac murmur and following thorough echocardiographic study their murmur was proved to be innocent were assigned as the control group. Corrected QT dispersion (QTcD) was measured in both groups (MVP and control). A three channel electrocardiographic recorder (Esaote, model P80, manufactured by SAG, made in Switzerland and distributed by Esaote S.P.A., Italy) was used. ECGs were recorded at a speed of 25mm/s and amplitude of 10mm/mv. The QT and preceding PR intervals of three consecutive sinus beats were measured in a range of nine to twelve leads17-19 The leads with flat ST-T waves were excluded from analysis.20 The QT and RR intervals were measured manually with calipers!
by a single observer. Thereafter repeatability of the QTcD measurements was tested by a second observer. QT interval was taken from the onset of the QRS to the end of T wave (i.e., return to the T/P baseline). If U waves were present, the QT interval was measured to the nadir of the curve between the T and U wave. The QTcD was calculated by the method of Bazett21 (QTc= QT
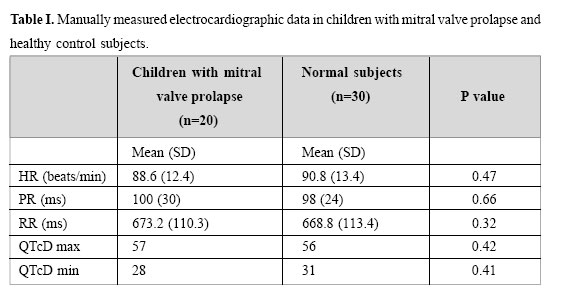
Data are expressed as mean± SD. Unpaired one-tailed Student’s t test was used for testing the difference between the two groups. A P value<0.05 was considered significant. None of our patients had ventricular arrhythmias on surface electrocardiogram. QTcD was 39±14.7 and 40±15.2 milliseconds in the two groups of control and children with MVP respectively. Mean values of the two groups were compared using unpaired Student’s t-test. The QTcD was not significantly different in children with MVP. Other ECG findings are mentioned in Table I. This study demonstrates that in children with uncomplicated isolated MVP, increased QTcD is not as frequent as in adults. Indeed none of our patients showed a significantly different QTcD in comparison with our normal children group. Ventricular arrhythmias are common in adults with MVP. PVCs and complex PVCs has been reported to occur in 58% to 80% and approximately 50% of adults with MVP respectively.8 Leclercq et al. reported ventricular arrhythmias in 70% of their patients.22 Various causes have been cited for the occurrence of ventricular arrhythmias, including autonomic dysfunction, papillary muscle traction, abnormal QT dispersion, mechanical stimulation of myocardium by leaflets, abnormal innervation of floppy mitral valve and so on.23 Babuty et al. evaluated 58 adult patients with MVP and concluded that the main determinant factors of complex ventricular arrhythmias in these patients are patient age and mitral regurgitation.15 Tieleman et al. studied 32 patients with echocardiographically documented mitral valve prolapse and showed that QT dispersion on the 12 lead surface electrocardiogram was greater in patients with MVP with ventricular arrhythmias than in normal controls.10 To our knowledge, there is no study that has specifically addressed the issue of QT dispersion in children with uncomplicated isolated MVP. Wroblewska – Kaluzewska et al. analyzed arrhythmia and ST –T abnormalities in children with mitral valve prolapse. Only one Another explanation might be sought in the real importance and clinical potential of QTcD. Malik et al. reported that although QT dispersion is increased in cardiac patients compared with healthy subjects and the prognostic value of QT dispersion has been reported, values are largely overlapping, both between healthy subjects and cardiac patients and between patients with and without adverse outcome.They added that QT dispersion is a crude and approximate merasure of abnormality of the complete course of repolarization.33 In conclusion, we found that QTcD in children with MVP does not differ significantly from normal controls. This may explain the low incidence of ventricular arrhythmias in this age period. Considering several reports of increased QT dispersion in patients with MVP,it seems that the abnormality of QT dispersion is a phenomenon that occurs over several years and is not a congenital electrophysiologic abnormality.
Copyright 2004 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr04019t1.jpg] |
| |||||||||
{kind=link}