 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
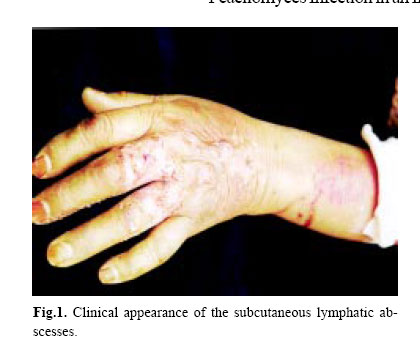
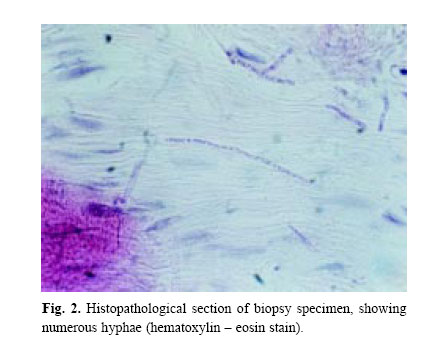
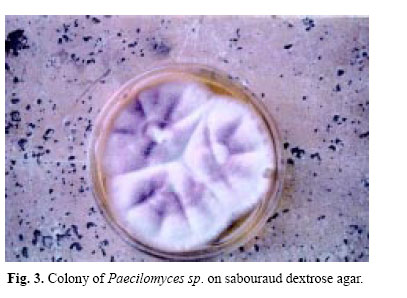
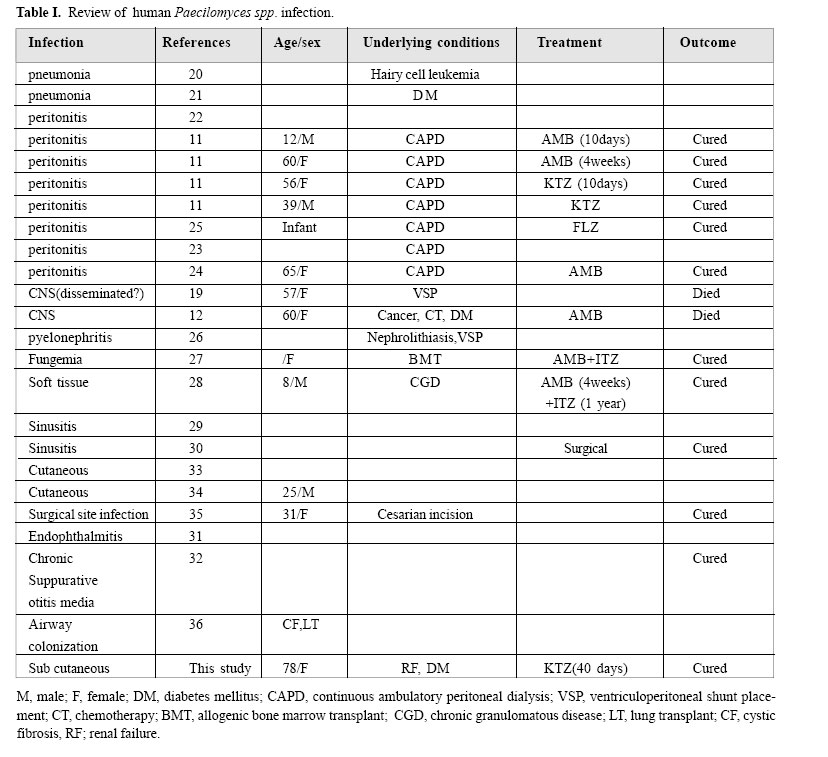
Medical Journal of the Islamic Republic of Iran , Vol. 18, No. 2, August, 2004, pp. 181-184 PEACILOMYCES INFECTION IN AN IMMUNOCOMPROMISED PATIENT From the Department of Medical Mycology, Pasteur Institute of Iran, Tehran, Iran. E-mail:shahindokhtbassiri@yahoo.com Code Number: mr04020 Paecilomyces sp. is a saprophytic fungus which has rarely been associated with human disease. We report the first case of invasive subcutaneous infection caused by this fungus in a 78-year-old female from Damghan, Iran, with diabetes and chronic renal failure. A biopsy provided an initial diagnosis of the mold in tissue. Multiple positive fungal cultures which were obtained from the biopsied tissue were subsequently identified by microscopic and macroscopic characteristics to be Paecilomyces sp. This case was successfully treated by oral ketoconazole (200 mg/day). Keywords: Paecilomyces infection – fungal infection – immunocompromised patients. INTRODUCTION Paecilomyces spp. is seldom associated with human infections. Most of the cases recorded have been of a mycotic keratitis. Several cases are now on record of endocarditis following valve replacement,1 and endophthalmitis following lens implantation.2 This common air-borne contaminant is resistant to most sterilizing techniques. Several nosocomial infections have occurred in which the organism was growing in the disinfectant used for surgical instruments. In that outbreak there were 12 cases of endophthalmitis following intraocular lens implantation2-3 The first case of endophthalmitis was reported by Uys4 in 1963, and it is typical of these cases. Paecilomyces was isolated from the blood, from a thrombus overlying the mitral valve, and from an embolus in the iliac artery following the death of a patient who had had a valve replacement.4 Paecilomyces spp. was recovered from the renal pelvis by Sherwood and Dansky, who reviewed Paecilomyces infections up to 1983.5 Pulmonary infusion6-7-8 and pneumonia9 have been noted. Georg et al.10 isolated Paecilomyces fumosoroseus from pulmonary lesion in a giant tortoise. Mycelium was present in many small abscesses throughout the lung. Most cases are cutaneous or concern transient catheter- related infections, but also deep infections are known.18 The present article describes Paecilomyces spp. from subcutaneous tissue in the insulin induction site. CASE REPORT The patient was a 78-year-old woman residing in Damghan, Iran, diagnosed with chronic renal failure and diabetes mellitus for a long time. The patient referred to the Medical Mycology Department, Pasteur Institute of Iran with pruritic, erythematous, edematous subcutaneous nodules of the left hand with adjacent suppurative lymphatics. His problem began 28 days before she refered to the Medical Mycology Pasteur Institute laboratory. Organisms had inoculated in the left hand in the insulin induction site. The patient had spiking fever and multiple subcutaneous abscesses in the left forearm (Fig. 1). Fever had started 12 days after her problem began. Urine culture and tissue culture for bacteria were negative . Her clinical history revealed that she had chronic renal failure over a period of 25 years and diabetes mellitus for over 14 years. She received insulin for 4 years befor her problem began. Biopsy specimens of the lesions were performed. Specimens were directly examined with 10% potasium hydroxide. The biopsy specimen showed hyphae (Fig. 2) The tissue sections were stained by hematoxylin and eosin and periodic acid schiff stains. Sections revealed a granulomatous reaction. Ground tissues were cultured on Sabouraud dextrose agar, sabouraud dextrose with chloramphenicol (50 mg/mL), blood agar and brain heart infusion agar (BBL); Duplicate cultures on each medium were incubated at 35oC and 25oC, cultures of specimens gave rise to Paecilomyces spp. Microscopic features of the isolates were studied by slide culture preparation. Paecilomyces colonies turned lilac in the substatum (Fig. 3). Microscopic examination showed hyaline septate hyphae similar to Penicillium spp., but the phialides are single or verticillate on well – developed conidiophores or directly on vegetative hyphae (Fig. 4). The phialides end in a long tapered tube and bear long chains of lemon-shaped or nearly cylindrical conidia. Chlamydoconidia and aleurioconidia are also produced. The patient was treated for 40 days with oral ketoconazole (200 mg/day). Paecilomyces spp. is a common fungus in the air and can grow in environments with high ambient temperatures. The fungus has been reported to be the causative agent of human mycoses in the literature, mostly occurring in conjunction with prosthetic implants or immunosuppression. Cases include pneumonia,20-21 peritonitis,11-25 a fatal infection of a ventriculoperitoneal shunt19 a case of pyelonephritis,26 fungemia,27 soft tissue infection of the heel,28 sinusitis29-30 endophthalmitis,31 chronic suppurative otitis media,32 cutaneus infection,33-34 and a mycosis at the incision site of a patient who underwent a cesarean section.35 Essential data are summarised in Table 1. Anderson et al13 described infectious complications in 80% of renal transplant patients or renal failure, associated with high-dose corticosteroid therapy, hyperglycemia, leukopenia, or age over 40 years. These risk factors operated presumably by effects on suppression of humoral and cellular immunity and impairment of polymorphonuclear leukocyte function.13 Our patient’s infection was caused by the opportunistic fungus Paecilomyces and was associated with three of the four risk factors noted above. Because the organism was demonstrated in the dermis in pure culture on two separate biopsies, we considered it etiologic in our patient’s infection. Many organisms that were previously considered to be contaminants when isolated from human specimens have emerged as major causes of disease, especially in the immunocompromised host.20 Our patient survived with antifungal treatment. This treatment included ketoconazole (200 mg per day) for 40 days. REFERENCES
Copyright 2004 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr04020f4.jpg] [mr04020f1.jpg] [mr04020f3.jpg] [mr04020f2.jpg] [mr04020t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}