 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
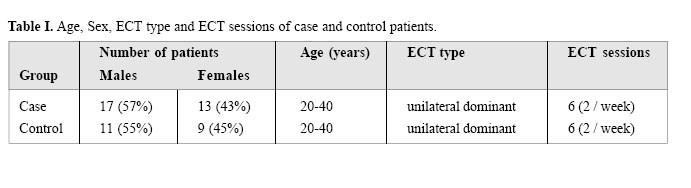
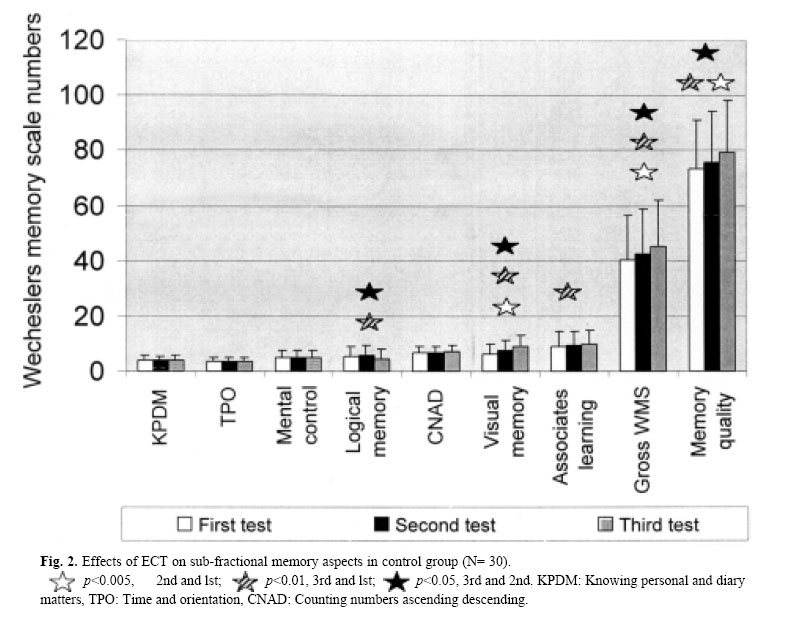
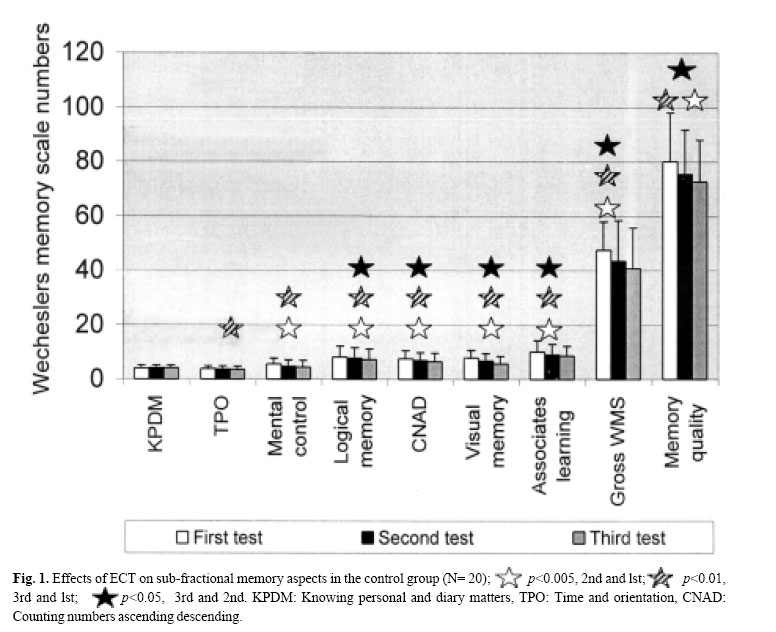
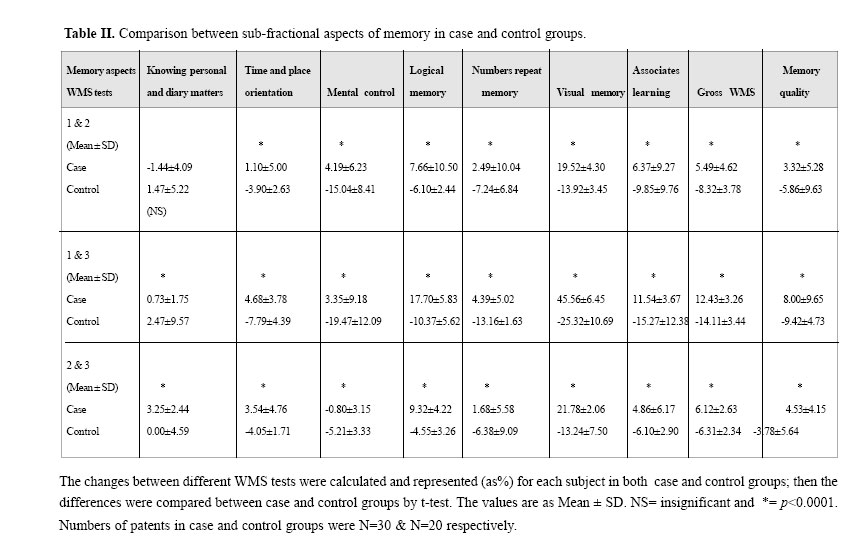
Medical Journal of the Islamic Republic of Iran , Vol. 18, No. 2, August, 2004, pp. 111-117, EFFECTS OF DESMOPRESSIN ON MEMORY DISORDERS DUE TO ELECTROCONVULSIVE THERAPY (ECT) IN HUMANS M-AL-R. HADJZADEH,*M.D., Ph.D., E. ABDOLLAHIAN, M.D., M.R. SARGOLZAIE, M.D., AND M.D. MOHEBBY, M.D. From the Department of Physiology and Avicenna Psychiatric Hospital, Mashhad University of Medical Sciences, Mashhad, Iran. *Corresponding author Code Number: mr04021 Electroconvulsive therapy (ECT) is an efficient treatment for several neuropsychiatric disorders; however a large number of patients develop memory impairment after ECT. Different studies both on animals and human suggest that vasopressin has positive effects on memory and improves cognitive functions. In this randomized, double-blind controlled clinical trial, 50 patients with psychiatric disorders who were candidate for ECT were studied. In the control group (20 patients) who received normal saline, ECT resulted in impairment in several aspects of memory such as: immediate memory, short term memory, visual memory, associate learning and memory quality. The sub-scores for most of the sub-fractional aspects of memory by WMS tests were decreased significantly by the 2nd and the 3rd tests (p<0.001 for most of the measured parameters). In the case group (30 patients), each patient received 60 µg/day (in 3 doses) desmopressin as intranasal spray; during the ECT treatment most of the measured parameters were increased significantly by the 2nd and the 3rd WMS tests. There were significant differences between the two groups for most memory scores (p<0.0001). The data demonstrate that desmopressin has protective and facilitating effects on memory impairment after ECT. Therefore, we conclude that desmopressin may be effective in the prevention of memory disorders by facilitating effects on memory and learning processes and may be used in patients who receive ECT for neuropsychiatric disorders. Keywords: Memory disorders, ECT, desmopressin, vasopressin. INTRODUCTION Learning and memory are completely critical for all living animals and have a key role to save them in different situations with changes in external or internal environments throughout their lives. In human beings memory and cognitive functions are also critically important for intellectual and social behaviors.1,9,11 Several causes may produce cognitive dysfunction and memory impairments, including: physical brain damages, cerebral infections, cerebral vascular disorders, senile dementia, chronic alcoholism, surgical operations on different brain regions, degenerative diseases of the brain, an array of hormonal disturbances and psychological drugs and procedures including electroconvulsive therapy (ECT).11,15 Electroconvulsive therapy is an efficient treatment for several neurosychiatric disorders such as major depression, mania, catatonia, Parkinson’s disease, neuroleptic malignant syndrome and mood disorders. ECT has been used in psychiatric hospitals since the 1940s and is routinely used nowadays for some patients.11,20 Although ECT is very effective, unfortunately a large number of ECT treated patients develop memory impairment and amnesia. These side effects in some patients may last for several weeks or sometimes a few months, which is a great problem for both patients and medical teams.11 Several studies both in animals and humans have demonstrated that vasopressin or its synthetic analogues have facilitating effects on learning and memory and are able to enhance learning and memory and affect amnesia due to ECT.3,4,5,9,24 Although these reports have indicated the beneficial effects of vasopressin, in both animal and human studies conflicting results have been reported. In humans the results of treatment with vasopressin with respect of memory improvement were reported to be inconsistent.10,18 On the other hand in our medical centers enough attention has not been paid to vasopressin effects on amnesia in patients who receive ECT; thus this study was performed to evaluate the possible impacts of desmopressin (DDAVP) on amnesia in patients following ECT. This study was performed from October 2001 to January 2002 in the Psychiatric Department of Avicenna Hospital, Mashhad, Iran. Only hospitalized patients, for whom ECT was selected as an effective treatment and were candidates for ECT were entered in this study. We also tried to cover some interfering factors such as: age, number of ECT sessions, ECT type, cognitive disorders such as dementia, and hormonal treatment. Patients were included by staff members and randomization was performed by a different one in the ward. During the memory tests the interviewers did not know if the patient belonged to the case or control group; nurses also didn't know if they were giving the patients drug or placebo. In this double - blind clinical trial study, 50 patients with psychological disorders who were candidate for ECT treatment were randomly divided into case (N=30) and control (N=20) groups. All people in both groups were between 20-40 years (mean = 29) and the type of ECT for all subjects was unilateral dominant and it covered 6 sessions (both groups were homogeneous for these factors). In the case group 17 male (M) and 13 females (F) and in the control group 11 M and 9 F were included. Each patient in the case group received 60 µg/day (in 3 doses) desmopressin (Dumex-Alpharma, Denmark) as intranasal spray and each patient in the control group received normal saline by the same manner for 15 days; i.e. one day prior and two weeks during ECT treatment.Serum electrolytes Na+ and K+ were assessed for both groups before desmopressin treatment and by the end of the study. ECT was performed by an instrument (DUO-Pulse, Electron LTD, England) with 26 pulse/s (67 joule) or 40 pulse/s (125 joule) for 1-6 s to induce convulsion, which should continue at least for 20 s. Each patient in both groups received 3 ECT courses/week for 2 weeks. For evaluation of memory impairments, Wechesler's memory scale (WMS) test was employed. Three courses of WMS test were performed for all subjects throughout the study. The first course one day before ECT treatment as the base test and the second one after the 3rd ECT session (the end of the first week) and finally the third test after the 6th ECT session (the end of the second week). The WMS test was performed when the patients had left the ECT room and their consciousness was stable which took about 2 hours. This test gives sub-scores for all aspects of immediate, short, long and visual memory. The most important sub-scales include: knowing the personal and diary matters, time and place orientation, mental control, logical memory, counting numbers ascending or descending, visual memory, associates learning, gross WMS score and finally memory quality. This scale gives the corrected score for patient's specific age beside the gross score. The results of each WMS test were represented as Mean ± SD, then analyzed and compared for each group by paired t-test, and for case and control groups by t-test and the differences considered to be significant when the P values were less than 0.05. This study covered 50 patients, 30 as case and 20 as control groups. Among the patients 28 (56%) were male and 22 (44%) were female. All patients were selected between the ages of 20-40 (Mean=29) and no significant differences were found between the 2 groups. Concerning the type of ECT and the number of ECT sessions all patients in both groups were treated in the same way; thus no differences were expected (Table I). Serum Na+ and K+ concentrations were in the normal range both before and by the end of the study for both case and control groups; no significant differences were found between the 2 groups. The results of WMS tests for case and control groups are demonstrated in Figure 2 and 1 respectively, while the comparison between the two groups are demonstrated in Table II. a) Case group: the sub-scores for "knowing personal and diary matters", "time and place orientation" and "mental control" were not significantly different between 3 tests (Figure 2). The sub-score for "logical memory" which was 5.48 ± 3.43 at the first test was increased to 5.90 ± 3.79 at the second and to 6.45 ± 3.63 at the third test.
The changes between WMS tests for the sub-scores for "mental control", "counting numbers", "logical memory", "visual memory", "gross WMS" and "memory quality" between case and control groups were significantly different (Table II). d) Sex related memory quality: sex related changes for "memory quality" in men and women for case and control groups are as follows: i) Case group: the percent of changes between the 2nd and the 1st test in men was 3.67 ± 6.55 and in women 2.70 ± 6.61 (NS). The changes between the 3rd and the1st test in men was 9.71 ± 6.24 while in women 5.30 ± 8.63 (NS) and finally the changes between the 3rd andthe 2nd test in men and women were 5.8 ± 6.43 and 2.50 ± 8.21, respectively (NS). ii) Control group: the percent of changes for "memory quality" between the 2nd and the 1st tests in men was -5.55 ± 4.12 and in women -6.27 ± 5.40 (NS). These changes between the 3rd and the 1st test in men and women were -9.40 ± 8.19 and -9.90 ± 3.51 respectively (NS), and finally between the 3rd and the 2 nd tests in men and women the changes were -3.70 ± 7.39 and -3.88 ± 2.78 respectively (NS). The differences between men and women in case and/or control groups were insignificant. In the present study we found that "knowing personal and diary matters" which is regarded as a long term memory didn't change after ECT in both control and case groups (Figure 1& 2); indicating that long term memory is unimpaired following ECT. The minimal changes (though significant) between the case and control groups (between 1 & 3 and 2 & 3 tests) that have been demonstrated in Table II, may be due to tiredness or anxiousness in subjects after ECT. The sub-scores for "time and place orientation" and "mental control" in the control group have significantly decreased after ECT (Figure 1), while in the case group they have increased (though insignificant) (Figure 2). The significant differences between the two groups for these sub-fractional memories (Table II) demonstrate that desmopressin in the case group had facilitating effects on these aspects of memory and may improve the memory impairments following ECT. In this study the "visual memory" in the control group has significantly decreased by -13.92% after the second and by -25.32% after the third WMS tests while in the case group an increase by 19.52% and 45.50% were seen respectively (Table II). This finding shows that short term memory is not well stabilized and it may be more impaired by ECT. On the other hand, these findings indicate the facilitating effects of desmopressin on visual memory. Visual memory as a short term memory was severely impaired by ECT in the present study and improved by desmopressin which is supported by Muller et al. who reported that desmopressin increased the short term memory in children with nocturnal enuresis.17 Our findings are also in agreement with that of Laczi et al. who reported the facilitating effects of desmopressin in patients with memory impairments without any defect in attention or consolidation.13 Till et al. also have reported that desmopressin has improved short term m! emory in patients by the first week of treatment; which is supporting our finding in the present study.22 Another finding of this study as has been shown in Figure 1 is the reduction of sub-scores for "logical memory", "counting numbers" and "associate learning" in control subjects; these data show that ECT has decreased the scores and has impaired all these aspects of memory in this group. Despite this, desmopressin has increased the scores and improved all these aspects of memory in the case group (Figure 2). Our finding is in agreement with those of Wingartner et al. who reported that desmopressin facilitates learning processes such as completing sentences, organization and retrograde memory following ECT.24 "Memory quality" in the control group was decreased after ECT (Figure 1), but in the case group it was significantly increased (Figure 2). The mean score changes in the control group decreased by -5.86% by the second and by -9.42% by the third WMS tests, while in the case group the increase was 3.32% and 8% respectively. These findings also show the protective and facilitating effects of desmopressin in memory quality after ECT. In regard of sex we found that memory quality decreased after ECT in both men and women in control groups, but the difference was insignificant; this may suggest that ECT can impair memory in both sexes, although the impairment is not sex-dependent. On the other hand, desmopressin had some facilitating effects on memory quality both in men and women. Although a 9% increase for men and a 5% increase for women were present, this wasn't statistically significant. Therefore, this finding indicates that desmopressin would improve memory after ECT! in both men and women in the same manner. Our finding is in contrast with that of Beckwith et al. who reported the facilitating effects of desmopressin on memory in men but not in women.2 This contrast may in part be due to the selective age group for women in our subjects who were between 20-40 years and their normal hormonal secretion may impact the outcome of desmopressin effects in women in our study. In this study sub-fractional aspects of memory with the exception of "knowing personal and diary matters" which is regarded as a long term memory was impaired after ECT in control subjects which is approved by several animal experiments4,5,16 and human studies.20,23 On the other hand, desmopressin had a protective and facilitating effect on different aspects of memory in the case subjects. All sub-scores in the case group have increased during treatment with desmopressin throughout the study which indicates that the effects on memory impairment persist with continuing of desmopressin treatment. Although it seems that the facilitating effects of desmopressin is not a hormonal effect,3 both V1a and V1b and also a sub-species of V2 vasopressin receptors are present in the brain.7,19 Vasopressin can bind with these receptors and may stimulate cholinergic mechanisms5 which have impact on memory or may act as neurotransmitter and stimulate the synthesis of biochemical agents, thus acting as a neuromodulator.1,8,19 The impacts of desmopressin on second messenger systems involved in memory processes such as calcium - calmodulin - protein kinase II and protein kinase A pathways and NMDA receptors in CA1region in the hippoc-ampus12,14 may in part be responsible for desmopressin effects on memory. Stimulating choline acetyltransferase activity in visual cortex, stimulating acetylcholine release and inositol - phospholipid metabolism in the hippocampus and promoting NGF gene expression in the hippocampus and cerebral cortex have also been reported to be involved for decompression effects on memory processes.21,25 This study confronted some limitations such as: i) The number of patients in each group due to limitation in the number of candidates for ECT; ii) The basic psychiatric disorder was not unique, which may interfere with the result; iii) The threshold of electrical stimulation for convulsion was different for each patient which again might have interfered with the results. Therefore, these limitations should be considered here. In conclusion, this study demonstrated that ECT could impair different aspects of memory in patients who receive ECT as psychiatric treatment. The main result of this study is that vasopressin and its analogue including desmopressin can facilitate learning and memory and have facilitating effects on different aspects of memory and also show protective effects on memory impairments after ECT. Therefore, we suggest that desmopressin may be used in patients who receive ECT for different psychiatric disorders to protect and improve memory impairments. This study was supported in part by a grant from the Conceal of Research, Mashhad University of Medical Sciences, and the authors would like to thank them for offering us the grant to finance this work. REFERENCES
Copyright 2004 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr04021t1.jpg] [mr04021f1.jpg] [mr04021t2.jpg] [mr04021f2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}