 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
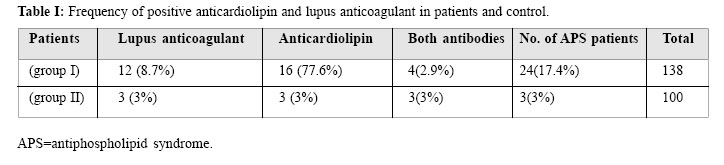
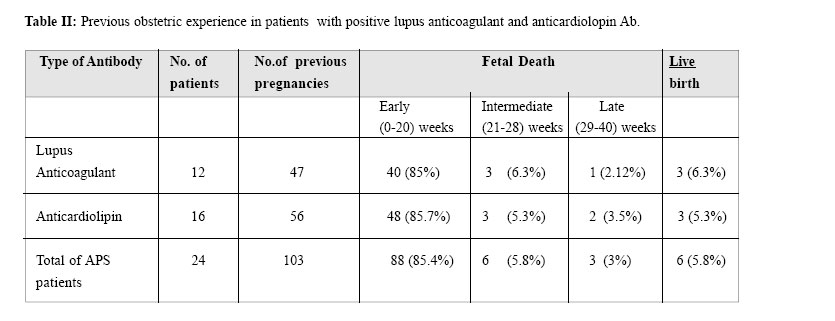
Medical Journal of the Islamic Republic of Iran , Vol. 18, No. 2, August, 2004, pp. 119-121 THE PREVALENCE OF ANTIPHOSPHOLIPID SYNDROME IN PATIENTS WITH RECURRENT PREGNANCY LOSS: A REPORT FROM SOUTH OF IRAN From the Department of Gynecology and Immunology, Shiraz University of Medical Sciences, Shiraz, Iran. Code Number: mr04022 In order to determine the role of different anti-phospholipid antibodies as an etiologic factor in recurrent pregnancy failure, a prospective study was done on one-hun-dred and thirty-eight women who had unexplained recurrent pregnancy loss (group I) with one-hundred well-matched women with normal reproductive outcome allocated as control group (GII). Sera from 138 patients and 100 controls were analyzed for anticardiolipin antibody (ACLA) and lupus anticoagulant (LA). ACLA was measured by Elisa and LA by activated PTT. Sixteen women (11.6%) had positive ACLA in group I, while 3 (3%) of group II were positive for this antibody (p= 0.0157 and odds ratio = 4.24). LA was positive in 12(8.7%) of group I and 3(3%) of group II, but the difference was not significant (p= 0.074, odds ratio=3.08). Overall 24 women (17.4%) were positive for one of the mentioned antibodies (p= 0.00055, OR= 6.81). Four patients were positive for both antibodies. This study emphasizes the relationship between antiphospholipid syndrome and recurrent pregnancy failure. Keywords: Anticardiolipin antibody, lupus anticoagulant, pregnancy loss. INTRODUCTION Recurrent pregnancy loss (RPL) is the loss of 3 or more spontaneous consecutive pregnancies.1 Recurrent miscarriage is a common problem in the United States. It affects more than 500,000 women annually. 2 There are many causes, such as genetic, anatomic, hormonal, medical and immunologic causes.2,3 If properly screened the cause will be found in almost all women.1 The most common singular defect in women with recurrent miscarriage syndrome is a hemostatic defect, and if a thorough antiphospholipid evaluation is performed, the most common of these is found to be antiphospholipid syndrome.1 Antiphospholipid antibodies (apl-ab) are acquired autoantibodies against a phospholipid that have been associated with slow progressive thrombosis and infarction in the placenta.3 Clinical features (venous or arterial thrombosis, recurrent fetal loss and thrombocytopenia) in conjunction with positive laboratory findings (positive IgG or IgM anticardiolipin antibodies (ACLA) or positive lupus anticoagulants (LA)), will satisfy the criteria for the diagnosis of antiphospholipid antibody syndrome.3,6 These women have only a 10% live-birth rate in subsequent pregnancies in which no pharmacological treatment is given.4,5 The purpose of this study is to find out the prevalence of different autoantibodies in patients with recurrent pregnancy loss of unexplained etiology. The study population were patients who referred to the abortion clinic of our university hospital between February 1998 and September 2001. Patients with a history of 3 or more previous pregnancy losses, or stillbirth not caused by infection, abruption and congenital malformation were included in the study. In the total 192 cases with recurrent pregnancy failure, the etiology of loss was investigated by complete work up such as karyotype, hysterosalpingography, infection studies, hormonal assay, and endometrial biopsy. As a result 138 patients remained with no etiology. In group I the age of the patients ranged between 18-39 years old and the number of previous losses were between 3-7. Control group consisted of 100 women with no previous fetal loss, who were matched with the study group (group II). The age range was 19-40 years old. Sera was taken from both groups for antibody measurement (twice with 6 weeks apart). Chi-square test was used as statistical analysis. The mean maternal age was 28.7 years in group I and 26.8 in group II. 16 patients in group I (11.6%) and 3 in group II (3%) were positive for anticardiolipin antibody, which has statistical significance. p= 0.01575, odds ratio= 4.24, C.I (95%)= (1.12, 18.88). Lupus anticoagulant which was identified by a prolonged activated PTT was also positive in 12 cases in group I (8.7%) while 3 patients in group II (3%) were positive for lupus anticoagulant. p= 0.07430, odds ratio=3.08, C.I (95%) = (0.78, 14.16). This was statistically of borderline significance. Overall 24 cases in group I (17.4%) and 3 in group II (3%) were positive for antiphospholipid antibody (p= 0.00055, odds ratio=6.81) (Table I). In group I four patients were positive for both antibodies. As shown in Table II most of the fetal losses in patients with antiphospholipid syndrome occur in the first half of pregnancy. As shown in Table II, overall among patients with antiphopholipid syndrome, the prevalence of fetal loss is more in the first trimester. The autoimmune cause of recurrent pregnancy loss involves two antibodies, lupus anticoagulant and anticardiolipin antibody. In the current study, we found a prevalence rate of anticardiolipin as measured by Elisa of 11.6% and lupus anticoagulant as ascertained by prolonged activated PTT to be 8.7% in patients with recurrent fetal loss and an overall prevalence rate of 17.4% was detected in the patient group. According to the study of Festin et al. in 1997 the rate of lupus anticoagulant is 7% and anticardiolipin is 15% among patients with previous fetal loss of unexplained origin.1 These two antibodies are believed to cause thrombosis in the maternal circulation leading to events that lead to fetal losses.1 The reports from other investigators show that the prevalence of antiphopholipid antibodies in the normal obstetrical population is 5.3% among 7278 women, while in patients with recurrent pregnancy loss this number was 20% among 2226 women.3 Another report by Charles et al. from the lupus unit in London showed a figure between 7% and 25% of antiphospholipid syndrome among British patients with recurrent fetal loss.7 On the other hand, some investigators do not agree with this relationship. As in reports by Vila et al, among 552 normal French blood donors, IgG anticardiolipin was found in 6.5%, and IgM anticardiolipin in 9.4%.8 Also in 1998 reports from Simpson et al. showed the lack of association between antiphospholipid antibody and first trimester spontanous abortion.8 So these investigators claim that although in some reports, the prevalence of antiphospholipid antibodies are higher in patients than controls, but actually the frequencies are only marginally greater than in the normal population.9 A good explanation for different reports may be due to lack of presence of a standard assay for measuring the antibodies. As shown by Rebar et al, qualitative positivity for IgG anticardiolipin antibodies ranged from 31% to 60% among kits tested; the range was 6% to 50% for IgM anticardiolipin antibod-ies.10 Overall general consensus supports the association between first trimester losses, adverse perinatal outcomes and positive antiphospholipid antibod So we recommend that every patient with a previous history of unexplained fetal losses be screened for these autoantibodies, although further studies on larger populations are necessary to prove this matter.
Copyright 2004 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr04022t2.jpg] [mr04022t1.jpg] |
| |||||||||
{kind=link}
{kind=link}