 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
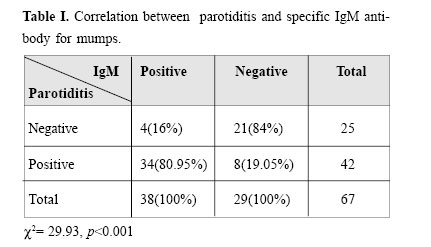
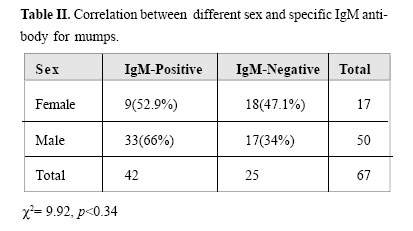
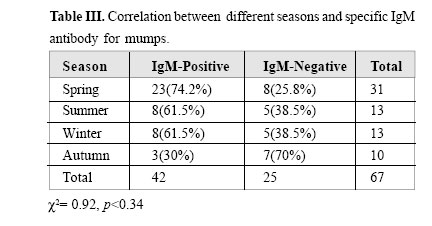
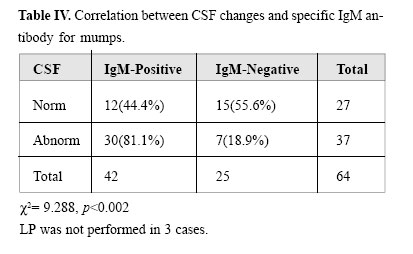
Medical Journal of the Islamic Republic of Iran , Vol. 18, No. 2, August, 2004, pp. 123-126 MUMPS MENINGOENCEPHALITIS IN PEDIATRIC WARD OF RASOOLAKRAM HOSPITAL IN TEHRAN, IRAN, 1999-2000 From the Department of Pediatrics, Rasool Akram Hospital, Iran University of Medical Sciences, Tehran, I.R.Iran. All correspondence should be submitted to: Dr. Samile Noorbakhsh, Iran University of Medical Sciences, Departement of Pediatric Infectious Diseases, Rasool Akram Hospital, Niayesh Ave, Satarkhan Street, Tehran, 14455, Islamic Repuplic of Iran, Email; saminoor@hbi.dmr.or.ir Code Number: mr04023 To determine the frequency of mumps infection in children hospitalized with aseptic meningoencephalitis (ME), as well as its correlation with parotiditis, this case-series study was conducted in the pediatric ward of Rasool Akram Hospital in Tehran, Iran, from 1999 to 2001. The blood samples of these patients were tested for specific IgM antibody for mumps by Elisa method. The results of this study showed that 62.7% of children with ME were IgM positive, and the remaining (37.3%) were IgM negative. There was a significant correlation between positive IgM and the presence of parotiditis. However, no correlation was noted between age, sex and season with IGM positivity except for CSF changes (aseptic meningitis) between the two groups. It can be concluded that the presence of neural symptoms (especially aseptic meningitis) in children less than 7 years of age with parotiditis could indicate mumps ME, especially in the spring. Due to a higher percentage of unvaccinated young persons <15yr old) in Iran, probably the incidence rate of mumps infection and its sequelae are higher compared with its incidence in developed countries before massive vaccination. Therefore with massive vaccination of Iranian young people (< 20yr old), the costs of! mumps infection and its sequelae will decrease. Keywords: Mumps infection; Meningoencephalitis; Mumps vaccination. INTRODUCTION Aseptic meningoencephalitis is an acute inflammatory process involving the meninges and, to a variable degree, brain tissue.1,2,3 Although the specific etiologic agent is not identified in most cases, clinical and research experience indicate that viruses are usually the responsible pathogens, accounting for seasonal pattern of disease. Enterovirus causes more than 80% of all cases. Other frequent causes of infection include arbovirus and herpes virus. Mumps is a common pathogen in regions where mumps vaccine is not widely used, in the below 15 year old group.1-8 The malignant form of ME is seen in 1/400-1/6000 cases of mumps, with 1.4% mortality.1,2,3 Specific IgM antibody for mumps virus is present in more than 75% of patients infected with mumps virus.1,2,3 There is no comprehensive report on the annual incidence rate of mumps and its role in ME of Iranian children, except for some seroepidemiological studies.5 In Iran, like other unvaccinated countries, with the peak incidence in children 5-9 years of age, 85% of infections occur in children <15 years of age, being almost rare in less than 2 yr old children.1-7 Mumps infection is endemic in Iran and mumps parotiditis is a common disease in Iranian children.4,5,6 However, in the United States, there has been a dramatic decrease in the incidence of mumps since the introduction of an inexpensive and very effective mumps vaccine in 1968.1,2,3,9-14 With regard to the role of this viral infection in affecting children and its consequences as well as the highest cost of hospitalization, the importance of massive vaccination against mumps virus should be recognized and emphasized in our country.15,16,17,18,19,20 The present study investigated the frequency of mumps infection in children with aseptic meningoencephalitis (ME) admitted to the pediatric ward of Rasool Akram hospital in Tehran, Iran during 1999-2000. This case-series study was performed on all children below 15 yr of age who were admitted to the pediatric ward of our hospital based on diagnostic parameters for aseptic ME. Inclusion-citeria for aseptic ME were fever plus one of the following symptoms (nausa& vomiting, headache, convulsion, confusion), signs of CNS involvement at the time of admission (positive meningeal signs; such as stiff neck, positive Krenig and/or Brudzinski sign), increased ICP, abnormal CSF finding, etc. Exclusion criteria were positive bacterial culture (blood, CSF or other site of body), or abnormality of CSF supposedly due to bacteral meningitis or another diagnosis except ME (space occupying lesion in brain, intracranial hemorrhage, etc.). Initially from each patient with ME, a questionaire was completed by the authorized physician, followed by clinical exams in the presence of neural symptoms and parotiditis. Two mL blood was drawn from each patient, blood samples were centrifuged and transferred to the research laboratory. The serum was estored in a -20 degree freezer until the serologic Elisa examination was performed on them. The evaluation of specific IgM antibody for mumps was carried out with commercial Elisa kits (Radim, Italy). The plate was read on an Elisa reader in 450& 620 nm wave length.The results were interpreted based on the manufacturer’s order. In this study, descriptional statistics (Mean, Standard Deviation), comprehensive statistics including Chi-square test for determination of correlation between sex, season, and parotiditis with positive IgM antibody (CI=95%) were used. Also, t-test was used to compare via SPSS 9 software. Sixty-seven patients were studied in two years.The age of patients was between 9 months to 14 years old (mean= 6.61±3.80) with a male to female ratio of 3/1. The highest incidence of ME was seen in the spring (31 cases= 48.8%) and the lowest in the autumn (9 cases= 13.4%). Abnormal CSF findings (aseptic meningitis) were present in 37(55.2%). Specific IgM antibody for mumps was reported positive in 1-13yr olds, mean7.36±3.38, sex ratio: 33/9, thirty three (34.2%) in the spring and the rest were observed in the other seasons. In this group 34(89.5%) had parotiditis and 4(10.5%) did not. Age of patients in the IgM negative group was between 1-14 years, mean 5.34± 4.72,sex ratio: 17/8. Eight cases (25.8%) occurred in the spring and the rest were observed in the other seasons. In this group 4(10.5%) had parotiditis and 21(72.4%) did not. There was a significant relation between positive IgM and parotiditis in patients (χ2 = 29.93, df= 1, CI=95%, p<0.001) (Table I). There was no significant difference between positive IgM and the negative IgM group in terms of age (two tail T-test= 1.98, p<0.067, 95% CI:-4.04-0.15); sex(χ2 = 0.92, df= 1, p<0.034) and season (χ2 = 5.11, df=3, p<0.164) (Table II, III, IV). Abnormal CSF was observed in 81% of positive IgM cases compared with 18.9% in the negative IgM patients (LP was not performed in 3 cases). There was a significant relation between positive IgM and abnormal CSF (χ2 = 9.288, p<0.002, df=1, CI=95%), (Table IV). Thirty-four patients (89.4%) with parotiditis (range 1.5-14 year, mean7.92± 2.89) were IgM positive, the remaining 4 patients (10.6%) were IgM negative, compared to 9 patients (31%) without parotiditis (age range 1-13 year, mean 4.96+4.29) who were IgM positive and 69% of the rest were IgM negative There was a significant age difference between patients with parotiditis and those without parotiditis (two tailed T-test= 3.32, significant=0.001). DISCUSSION ME is the most frequent complication of mumps infection in childhood.1,2,3,6,7,8 Its true incidence is hard to estimate because subclinical infection of the CNS, as evidenced by CSF pleocytosis, has been reported in In the United States, there has been a dramatic decrease in the incidence of mumps since the introduction of the mumps vaccine in 1968. In 1966, 628 cases of encephalitis due to mumps infection were reported with death in 10 cases of mumps. In 1987 there were 683 reported cases of mumps (0.27/100.000 population), a>99% reduction from the 152,209 cases reported in 1968. ME is now the 7th cause of encephalitis in the United States.1,2,3,5 The malignant form of ME is seen in 1/400-1/6000 cases of mumps, with 1.4% mortality. 1,2,3,8,9,10 Specific IgM antibody for mumps is present in more than 75% of patients infected with mumps virus.1,2,3,4 In Iran, due to the absence of mass vaccination of the population, mumps infection is present endemi-cally.4,5 Previous seroepidemiological studies by Hadian tibody for mumps. and Bahrami showed that the 0-9 yr old age group was most susceptible to mumps infection; followed by the 10-19 yr old age group. In the year 2000, Vojgani et al. showed that children below 5 yr of age were the most susceptible to mumps (p<0.05) and older than 10 year were the least susceptible group to mumps infection with no sex differences. In general, about 50% of the population have a tendency for mumps infection.21 Mumps is considered as one of the prevalent and important causes of aseptic ME in children, causing hospitalization in some cases.5 In another study conducted by Moddares et al., enteroviruses were the causative agent in 15% of viral ME below 1 years old; and mumps in 48% of patients below 14 years of age with the highest prevalence in 5-9yr old children. The lowest incidence of mumps ME was in <1yr of age (2.8%) and the sex ratio was 3/1. The highest seasonal prevalence was in the spring (53.5%), and parotiditis was seen in 79% of patients with mumps ME. The highest incidence of mumps M.E was 250/ 100,000. The results of this study, similar to Moddares et al.’s study showed that 62.7% of children with ME (9 mo-14 years, average 6.69 years) were positive for specific anti mumps-IgM (mumps infection). The rest (37.3%)were IgM negative (no mumps infection) probably due to other causes of ME or inadequate antibody response to mumps infection. There is no significant difference of age, sex and season, but a significant difference in CSF changes between the two groups. So in patients with ME, CSF changes are in favour of mumps ME rather than other viral causes. In this regard due to the similarity between the age distribution of ME patients with parotiditis and seropositive (IgM) patients, it can be concluded that the presence of neural symptoms (especially aseptic meningitis) and parotiditis in parallel in unvaccinated children with average age of~7yr could be indicative of mumps ME especially if it happens in the spring (CI 95%). The population of children less than 15 years old in Iran is about 24 million. Potentially, they are susceptible for mumps infection and are at risk of CNS involvement. In the presence of mumps ME without parotiditis (which is not always clinically diagnosed as mumps ME), some patients need hospitalization for decreasing their symptoms or definite diagnosis (ruling out bacterial meningitis). It is expected that the yearly incidence of mumps ME would be much higher in Iran compared to developed countries (before vaccination). Moreover, a higher percentage of unilateral sensory hearing loss in children is due to mumps or rubella virus.1,2,3,22 Considering the days of hospitalization and its costs for diagnosis, treatment, long term sequelae, and probably mortality which burden the health and medical system of our country, this disease is preventable by simple massive vaccination of young people below twenty years of age in Iran.
Copyright 2004 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr04023t1.jpg] [mr04023t3.jpg] [mr04023t2.jpg] [mr04023t4.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}