 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
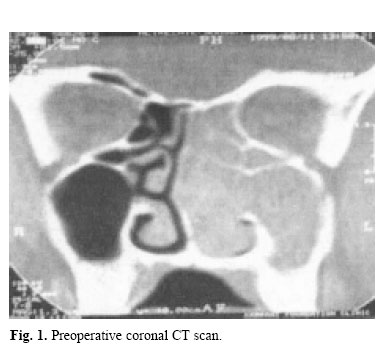
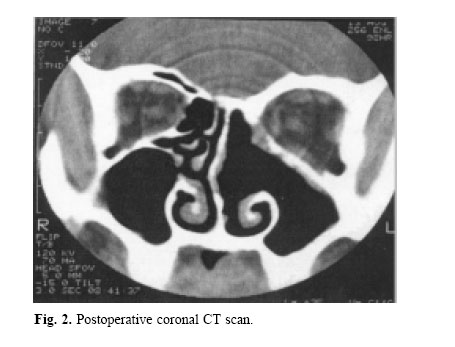
Medical Journal of the Islamic Republic of Iran , Vol. 18, No. 2, August, 2004, pp. 127-130 TRANSNASAL ENDOSCOPIC APPROACH FOR SINONASAL INVERTED PAPILLOMA MOHAMMAD HOSSEIN BARADARANFAR, M.D., AND PAYMAN DABIRMOGHADDAM, M.D. From the Department of Otolaryngology, Head and Neck Surgery, Sadoughi Hospital, Yazd University of Medical Sciences, Yazd, I.R. Iran. E-mail: baradaranf@ hotmail.com. Mailing Address: No 70, Laleh Alley, Kashani Street, Yazd, I.R. Iran. Zip code: 8916758385. Tel: + 98 351 5225291, Fax: +98 351 8224100. Code Number: mr04024 Inverted papillomas of the nose and paranasal sinuses are uncommon neoplasms, characterized by their tendency to occur and by their association with malignancy. In the past decade there has been a trend toward the use of endoscopic surgical techniques in the management of these tumors. This article presents the results of a prospective study of 24 patients with inverted papilloma resected by the endoscopic approach. 21 patients had unilateral disease and three patients had bilateral involvement. None of the patients had orbital or cranial extension. No association with malignancy was seen. Following endoscopic surgery, four patients had recurrences that required surgery. No complication occured in any of the patients. The results of endoscopic surgery for inverted papilloma is much better than nonendoscopic transnasal approaches and compares favorably with radical extranasal approaches. Endoscopic surgery is an effective surgical option for inverted papilloma removal. Keywords: Inverted Papilloma, Endoscopic Surgery, Paranasal Sinus Neoplasm. Inverted papilloma is a benign neoplasm that represents less than 4% of sinonasal tumors.1 It arises primarily in the nasal cavity but often enlarges to invade the lacrimal system, the orbit, or the intracranial cavity and can cause extensive destruction of bone and soft tissues.2 Lesions tend to be bulky, polypoid and characteristically pale pink to gray in color.3 Histologically the neoplastic epithelium inverts into the underlying stroma rather than proliferating outward and may invaginate to remodel bone but will not invade it without malignant transformation.4 The exact etiologies of inverted papilloma remain unknown, although a number of etiologies have been proposed including allergy, occupational exposure and chronic inflammation.4 A possible viral origin by Human Papilloma Virus (HPV) has repeatedly been reported by several authors5,6 although the frequency of virus particle finding was variable. Computed tomography (CT) is commonly used for the standard preoperative workup to evaluate the degree of involvement by tumor and to determine the extent of surgery.7 However it is difficult to differentiate neoplasm from inspissated mucus, mucoperiosteal thickening, or polyps resulting from obstruction of the sinus drainage pathways.8 Inverted papilloma is renowned for it’s high local recurrence rate and malignant transformation potential.9 The reported average recurrence rate ranges from 4%10 after radical extranasal excision to 66%11 after nonendoscopic endonasal excision. A review of literature showed that the overall association with malignancy is nine percent.12 It may be synchronic or metachronic.1 This study evaluates the presentation, treatment and subsequent clinical course of patients treated for inverted papilloma by the endoscopic approach. 24 cases of inverted papilloma were operated at the Amiralam hospital, Tehran and Rahnemoon hospital, Yazd between 1998 and 2003. 21 patients were managed with the transnasal endoscopic approach alone and in 4 other cases a combined approach (endoscopy with Caldwell-Luc) was performed. Histopathologic evaluation proved all cases to be inverted papilloma without any evidence of malignancy. Age at diagnosis, gender, presenting symptoms, site of lesion, primary versus recurrent treatment, endoscopy alone with or without the Caldwell - Luc approach and recurrence rates were reviewed. All patients were assessed preoperatively by endoscopic examination and coronal computed tomography (CT) imaging (Fig.1). Endoscopic resection was performed under general anesthesia. The nose was prepared using gauze soaked in solution of 2% lidocaine and 1:100,000 adrenaline. At operation an incision was made at the superior margin of the tumor and its attachment to the middle turbinate or lateral nasal wall was cut. Then the tumor was dissected toward the rostrum of sphenoid, inferior to fovea ethmoidalis with an elevator. An inferior incision was made at the junction of the lateral nasal wall and nasal floor and then an osteotomy was performed toward the posterior wall of the maxillary sinus. The anterior part of incision extends from the anterior attachment of the middle turbinate to the anterior part of the inferior turbinate and then connects to the inferior meatus. Depending on the tumor extension, the anterior margin of tumor resection may extend toward the ascending process of the maxilla or may include the nasolacrimal duct but this is unnecessary in all patients. The tumor with its surrounding soft tissues was medialized and then was pulled out from the nose. Resection of the medial orbital wall or inferior turbinate was performed in cases with involvement of these areas (Fig.2). All patients were regularly followed up and examined endoscopically with all suspicious areas being removed under local anesthesia and sent for histological analysis. Recurrences were resected under general anesthesia either endoscopically or via a combined (endoscopic and Caldwell - Luc) approach. The clinical data of the patients is presented in Table I. There were two female patients and the other patients were male. The mean age was 58.6 years with a range of 46 to 76 years. There were 13 (54%) left sided lesions and 8 (33.5%) right sided lesions with three (12.5%) bilateral lesions. The mean follow-up for all patients was 31.3 months with a range of 8 to 62 months. The most frequent symptom was nasal obstruction that was seen in 86% of patients. Other frequent symptoms were rhinorrhea (64%), headache and facial pain (36%) and epistaxis (15%). All patients were operated for the first time and no patient had malignancy associated with his disease. The diseased sites included the lateral nasal wall and adjacent sinuses without any orbital or cranial involvement. In two patients in which the site of attachment was the medial orbital wall, the involved portion was resected. Or bital, intracranial or lacrimal apparatus involvement were not seen.
Four patients with lateral maxillary wall involvement underwent endoscopic medial maxillectomy with the Caldwell-Luc approach. Sixteen percent (4/24) of the patients had recurrences after initial endoscopic resection which occurred within the first postoperative year. One of these was successfully resected endoscopically under general anesthesia and three required removal via a combined (endoscopy with Caldwell Luc) approach. None of the patients had residual disease at the end of this review. No complications were encountered in any of the patients. Because of the aggressive nature of tumor growth and malignant transformation potential, inverted papilloma should not be managed as a totally benign tumor. Inverted papilloma occurs most commonly in the fifth to seventh decade4,11 as shown in our study with a mean age of 62 years. A male predominance similar to our series is generally reported, with male to female ratios of 2:1 to 3:1.4,11,12 The most common presenting symptom is that of unilateral nasal obstruction12 which varies from 64%13 to 81%14 in the literature. Definitely inverted papilloma treatment is surgical and must aim at being radical.12 The radical external approach, lateral rhinotomy or midfacial degloving with en bloc resection of the lateral nasal wall, still remains the golden standard for inverted papilloma surgery due to the lowest rate of recurrence.9 The fact that most recurrences occur early and at the site of the original tumor strongly suggest that incomplete local resection is the cause of recurrent disease.9 Endonasal surgery was formerly performed without any endoscopic control and was known as conservative surgery. It was characterized by a very high recurrence rate ranging from 10% to 77%.1 The recurrence rate of the endoscopic approach is much lower than that of the nonendoscopic approach.9 This is attributable to the improved visualization of the tumor and anatomy, advanced surgical instrumentation and application of new techniques. It is noteworthy that the recurrence rate of the endoscopic approach is still higher than radical extranasal approaches.9 Our recurrence rate of 16% in this study is higher than that of radical extranasal excision that reflects certain limitations associated with the endoscopic approach but it compares favorably with other endoscopic series.1,3,9 It is important to note that endoscopic tumor surgery is technically demanding and associated with potential com-plications.15 To ensure a low recurrence rate and avoid complications, endoscopic tumor resection should be performed by surgeons who are experienced in the techniques of endoscopic sinus surgery.9 The endoscopic approach alone can be applied to tumors affecting the turbinates, ethmoid sinuses, and limited involvement of the maxillary, frontal and sphenoid sinuses. More extensive disease requires extranasal approaches which may be combined with the endoscopic approach at any time. The assessment of endoscopic resectability depends on preoperative endoscopic examination, CT imaging and more importantly intraoperative assessment including tumor visualization and accessibility. The role of endoscopy in the follow-up of these patients is important. The excellent visualization of the postoperative cavity enables early detection of residual disease. Furthermore minor revision surgery can be performed under local anesthesia as an outpatient procedure. In unilateral nasal obstruction or unilateral nasal polyps should alert the otolaryngologist to the possibility of inverted papilloma. Our results show that inverted papilloma surgery under endoscopic control is a satisfactory option in the armamentarium of treatments although it requires larger patient populations and longer follow-up periods for more definite evaluation.
Copyright 2004 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr04024f2.jpg] [mr04024f1.jpg] |
| |||||||||
{kind=link}
{kind=link}