 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Medical Journal of the Islamic Republic of Iran , Vol. 18, No. 2, August, 2004, pp. 131-134 EMBOLECTOMY FOR ACUTE LOWER LIMB ISCHEMIA From Shohada Tajrish Medical Center, Shahid Beheshti University of Medical Sciences, Tehran, I.R. Iran. *Assistant Professor of Surgery, Vascular and Trauma Surgery Department,
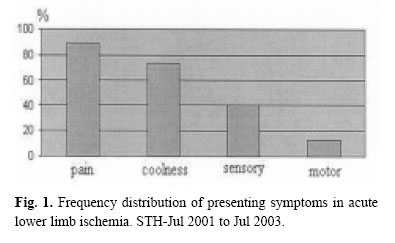
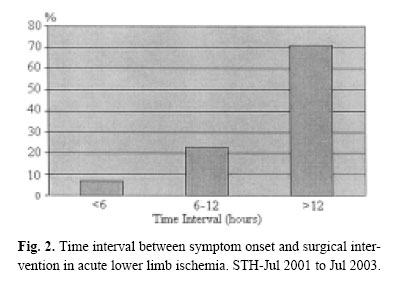
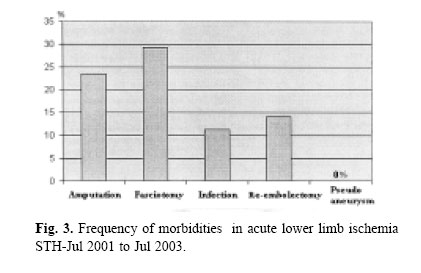
Shohada Tajrish Hospital Code Number: mr04025 In this prospective descriptive study, all patients with acute lower limb ischemia who presented to Shohada Tajrish Hospital (STH) between July 2001 and July 2003 were analyzed and followed for 6 months. The total population of 109 patients, with no significant difference in sexual distribution had a mean age of 64±16 years. 23% had AF and 31% had a history of MI, but in the ECG of 30%, no pathologic finding had been detected. Pain and coolness were the two most prevalent symptoms. Only one-third of the patients had normal sensory and motor examination in their limb and the rest had different degrees of impairment. More than 70% of the patients arrived here after 12 hours from the onset of the symptoms. Fasciotomy was done in 29%, and amputation in 23.5%. The mortality rate was 12.2%. Surgical site infection occurred in 11% and 14.1% underwent re-embolectomy. There was no pseudoaneurysms. The time interval from the onset, sensory and motor findings, and calf tenderness a! ffected the prognosis. Prognosis was better in smokers. The iatrogenic group which consisted of 13.7% of our patient population had the best prognosis (no mortality or morbidity). 4% of the patients who had first undergone embolectomy in other centers, all lost their limbs. In cases of late embolectomies, venotomy and heparin flush has lowered the amputation level without increasing mortality. Early referral by a cardiologist, receiving heparin rapidly and smoking are among the factors which improve prognosis. Keywords: Acute ischemia; Embolectomy; lower limb. INTRODUCTION Acute limb ischemia, with a prevalence of 1.7 in 10.000 general population,1 still has a high mortality and morbidity despite recent new techniques. Newer therapeutic methods are being used more frequently nowadays.2,3 During the course of this disease, several factors lead to increases in morbidity, such as fasciotomy due to prolonged ischemia, which has been reported in up to 48% of cases.4 Amputation rate had been 5-28% and that of mortality had been 7-25%.5,6 Previous studies have shown that, the interval before surgical intervention (more than 24 hours), calf tenderness, and presence of sensory and motor deficits have been associated with poor prognosis.4 The most common etiologies are cardiac diseases (80- 90%), among which atherosclerosis has replaced rheumatic diseases (60-70%).7,8,9 AF (Atrial Fibrillation) is diagnosed in one-half to three-fourths of the patients.8,10 In some studies up to 45% of emboli were iatrogenic (85% during angiography and 15% due to surgical approaches). 11 Axial vessels are the most common destination for the emboli (70-80%), among which the femoral bifurcation is the most prevalent (35-50%).12 Collateral vessels are among the important prognostic factors. Some of the complications are related to prolonged ischemia, such as amputation or fasciotomy, while others may be due to the underlying disease or surgical intervention, such as pseudoaneurysm, surgical site infection, fasciotomy site infection and re-embolectomies. In this descriptive, prospective study, all of the patients who presented with acute lower limb ischemia to Shohada Tajrish Hospital (STH) between July 2001 and July 2003, were analyzed. The criteria for entrance to the study were acute onset of ischemic symptoms, which sometimes had developed on a chronic basis. A questionnaire was filled for each patient, consisting of general personal information, age, gender, race, presenting symptoms (sensory, motor or calf tenderness) and their severity. Time interval from the onset to admission was notified. Previous illnesses, especially cardiac were recorded. ECG findings were also recorded. Saddle emboli (simultaneous involvement of both lower limbs) were omitted. Patients were followed during that admission and then during a 6 month interval. Complications such as re-embolectomy, wound infection and pseudoaneurysm were noted. Mortalities, amputations and their level were recorded. During the procedure of embolectomy, vascular exploration was done using local anesthetics (2% lidocaine, diluted) and with a femoral incision; and the embolectomy itself was done using an appropriate Fogarty catheter. Arteriotomy has always been longitudinal and then closed with 6-0 prolene continuous sutures. A closed suction drain was fixed for all of the cases and all received cefazolin : 1gr/IV beginning half an hour before the procedure and every 6 hours thereafter, while having a drain. All of the patients were fully anticoagulated. In cases of late embolectomy with calf rigor, a femoral venotomy was performed and the limb circulation was flushed with heparin, to reduce releasing toxins to the systemic circulation and lower the amputation level. Collected data were analyzed with SPSS software. Our study included 109 patients. Three did not come for follow-ups and 2 were excluded because of unreliable examinations. 93% of our patients had been referred to us. Sexual distribution was similar (51.8% female, 48.2% male) and 66% were older than 60, while only 8.4% were younger than 40 (mean age 64±16). AF was detected in 23.5% and MI in 31% (12% were recent MIs). In the ECG of 30%, no significant pathology was detected. The most common presenting symptoms were pain and coolness (Fig. 1). One third of the patients had normal sensory and motor examination. In 42%, sensation was decreased and in 27% was absent. 22% had decreased motor function and 38% had limb paralysis. Most of our patients arrived here after the golden time of 6-8 hours (Fig. 2). 24.5% of our patients were smokers. 22.6% had associated chronic ischemia and 26.4% were diabetic. The amputation rate was 23.5% (10.3% below knee and 13.2% above knee) and fasciotomy was done in 29.2% of cases. Some of the latter lost their limbs later. We had no pseudoaneurysms. All morbidities (related to ischemia itself or embolectomy) are shown in Fig. 3. The mortality rate was 12.2% and 76% of those who died, arrived to the hospital after 12 hours. After analyzing the results, a complicated limb was defined as one which had undergone fasciotomy or had been amputated (according to gross outcome not minor complications). Using this definition the relation between ischemic time and complicated limbs was significant (chi-square test : p= 0.0273). The same relation was detected between sensory and motor findings and clinical outcome (p= 0.0038 and p=0.0187, respectively). Using Fisher test, calf tenderness was related to amputation (p<0.001). There was no correlation between complications and underlying diseases (diabetes, chronic vascular diseases and smoking). Although fasciotomy was done less in smokers (p= 0.0151), the overall prognosis was better in smokers (p= 0.0203). In prolonged ischemia (more than 12 hours), limb salvage was possible in half of those with presumed below knee amputation on admission (6.5% of prolonged ischemia). 13% of those in which a hip disarticulation was presumed inevitable on admission, had a well-healed above knee amputation stump, on discharge. No difference in amputation and mortality was seen in different sexes. In the subgroup of iatrogenic ischemia (13.7%), we had no mortality or morbidity. 4% of our patients who had undergone embolectomy in other centers and were then referred to us, all lost their limbs. The fact that 93% of our patients were referral shows the importance of improving our outcome on national results. Only 23.5% of our patients had AF which is much lower than previous published figures.8,10 More than 70% of our patients arrived here after the golden time. This might be due to being a referral center. Following technical issues strictly may be the reason of the absence of pseudoaneurysms. Other complications have also been in an acceptable range. Underlying diseases have not increased the complications. Amputation rate had been similar to some of the recent studies,13 although some discrepancies,14,15 which were once significant,16 were noted. The mortality rate of 12.2% is significantly lower than some published re-ports.14,15 As previous studies had shown, sensory and motor findings, calf tenderness and time interval before intervention influences the outcome. In late embolectomies, venotomy and heparin flush had improved the outcome. Smokers had better results in our study. Although they consisted of only ¼ of our patients, and it might be hasty to have a definite conclusion, collateral vessels may be better in this subgroup. Although some studies show a prevalence of 45% of iatrogenic ischemia, we had only 13.7 % in this subgroup. It is interesting that this group which was almost always referred by cardiologists and after angiography and interventions, had no mortality and morbidity despite valvular and coronary artery disease. The smaller figure may be because of the less frequent endovascular interventions in our country and better results may be because of the rapid referral and initiation of anticoagulants. The results were worst in those 4% who previously underwent exploration and embolectomy in other centers. Although the 1st surgeon’s inexperience can be the cause as uncomplicated patients are not referred there is a bias in this conclusion. According to another study which was performed in our center 8 years ago, we had a 12-fold increase in patient number. Our mortality and morbidity had been acceptable and in comparison with some of the previous works, more encouraging. We had more idiopathic or unknown cardiac causes in our population. Besides the aforementioned prognostic factors, iatrogenic causes referred by a cardiologist and smokers had a better outcome. Using heparin for irrigation of the limb, in prolonged ischemia, had lowered the amputation level and simultaneously had not increased the mortality.
Copyright 2004 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr04025f2.jpg] [mr04025f1.jpg] [mr04025f3.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}