 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
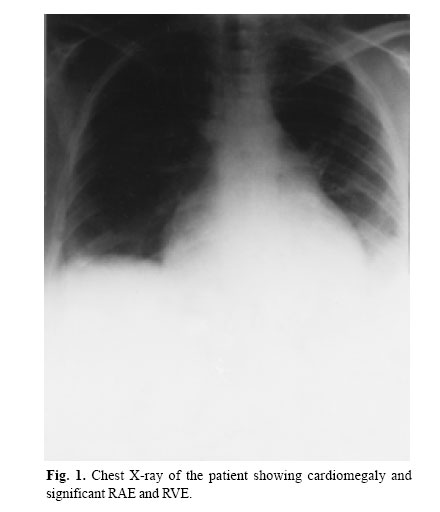
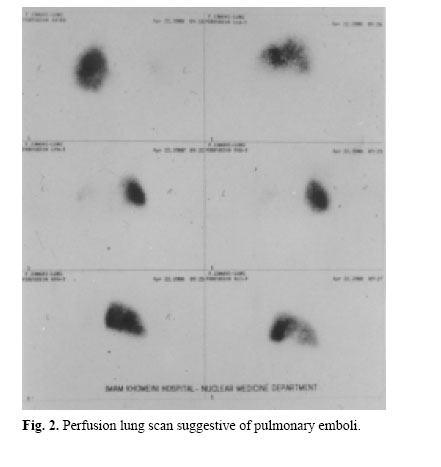
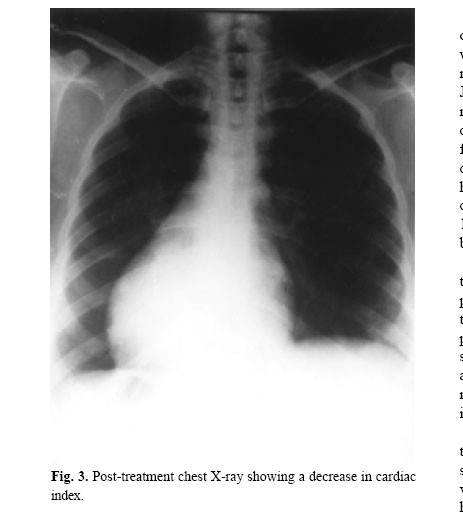
Medical Journal of the Islamic Republic of Iran , Vol. 18, No. 2, August, 2004, pp. 173-176 A CASE REPORT OF VASCULAR COMPLICATIONS, HEMOPTYSIS AND COR PULMONALE IN BEHCET’S DISEASE ALI KHALVAT,* M.D., AND REZA NAJAFIZADEH,* M.D. From the Dept. of Rheumatology, Imam Khomeini Hospital, Tehran University of Medical Sciences, Tehran, I.R. Iran. Code Number: mr04032 ABSTRACTA 33-year-old female-a known case of Behcet’s disease- was admitted to the hospital due to fever, dyspnea and hemoptysis. One week before admission, she had developed right leg swelling. The history suggested either deep vein thrombosis (DVT) and pulmonary emboli or pulmonary artery vasculitis. Diagnostic tests were requested and the necessary treatment was started accordingly. Keywords: Behcet’s disease – Vascular complication – Thrombosis – Vasculitis. INTRODUCTIONBehcet’s disease is a systemic vasculitis of unknown etiology with a definite and peculiar geographic distribution. Most cases are clustered around the countries of the Mediterranean basin, the Middle East and the Far East, characterised by a multisystem disorder of vasculitis type. Vascular complications are in three forms, systemic arterial vasculitis, pulmonary arterial vasculitis, and venous systemic involvement. The basic pulmonary pathology in Behcet’s disease is also related to vasculitis. Pulmonary vascular changes in the form of arterial aneurysms, arterial and venous thrombosis, and pulmonary infacts are found. These vascular complications are due to obstruction in venous and arterial flow. CASE REPORTA 33-years-old female was admitted to the Infectious Disease Ward of Imam Khomeini Hospital, Tehran, Iran, with fever, dyspnea and hemoptysis. The symptoms had appeared suddenly one day before admission. She also had a history of right leg swelling at about one week before that day. The history suggested DVT and pulmonary emboli so the patient was empirically treated with heparin. The patient had a history of recurrent oral and genital aphthae, so we asked the Rheumatology Department for consultation. In 1995 (5 years before the recent admission), the patient had been treated with colchicine because of Behcet’s disease manifestations (recurrent oral and genital aphthae, erythema nodosum and pseudofolliculitis). At that time, the pathergy test had been negative and ophthalmic examination was reported to be normal. As her mucocutaneous manifestations improved with colchicine, she discontinued taking the medicine on her own 4 years ago and didn’t come for follow-up visits from that time. In her past medical history, she had been operated upon 5 years ago because of a bicornuate uterus and 3 years ago because of ovarian cyst. She also reported an intrauterine fetal death at about 11 years ago. In physical exam, blood pressure was normal but tachycardia and tachypnea were noted, conjunctivae were a bit pale and her JVP was elevated. In chest exam, mild retraction of inter and subcostal and supraclavicular muscles were noted. Diffuse wheezing and some mild crackles in basal lung fields were auscultated. We detected a long S2 and a II/VI systolic heart murmur in the left sternal border too. Examination of the abdomen revealed bilateral collateral vessels draining upward. With a span of 14cm, the liver was palpable and extended 3cm below the costal margin. The spleen wasn’t palpable. No ascites was detected. In examining the extremities the right lower limb was swollen from lower thigh down to the leg with a 1 inch difference in diameter between the two legs. Peripheral vessels and their pulses were symmetrically palpated, the left breast was moderately tender with mild swelling and erythema but no discrete mass was detected by deep palpation. In ophthalmoscopy, mild tortuosity of retinal vessels was detected. Peripheral and cranial nerves showed no abnormality in examination. Laboratory and radiologic investigations revealed the following remarkable results (other related tests which are not mentioned were normal) WBC: 8500, P: 63%, L: 31% Hb: 12, ESR: 16, CRP: 4+, ANA: Neg., Anti DNA: Neg, LE Cell: Neg, ANCA: Neg, Anti-cardiolipin antibody (IgG-IgM): Neg, VDRL: Neg, PT, PTT: normal. ABG: PaO2 = 65, O2 Sat= 92%, pCO2 = 21, pH=7.45, ECG: right axis deviation, right atrial enlargement, right ventricular enlargement. CXR: Cardiomegaly, significant RAE and RVE (Figure 1). Echocardiography: RA& RV dilatation, paradoxical septal motion, TR++ PAP= 80mmHg, EF= 58%. Doppler ultrasonography of lower limbs: thrombosis of right superficial and deep femoral, right external iliac and right popliteal veins. In order to confirm the last abnormal finding, lung perfusion scan was requested which revealed a severe decrease in left lung perfusion and non-segmental defects in the right lung (Figure 2) which highly suggested pulmonary emboli. Abdominal ultrasonography: hepatomegaly was detected but the spleen and kidneys appeared to be normal. No para-aortic adenopathy was noted. During her admission in the hospital, she developed hoarseness and the ENT consultation revealed complete paralysis of the left vocal cord. Considering her PMH and present illness the most probable diagnosis was pulmonary emboli and DVT complicating Behcet’s disease. She was treated with heparin 24000 Units/day and after that warfarin was started with the required dose, too (INR: 3). A similar complication in the arterial system was probable, too, so pulmonary artery angiography was requested. Considering vascular complications and the inflammatory nature of the disease, prednisolone (30 mg/daily) was started to control the main offending disease, to be tapered quickly within a few months. During treatment, her dyspnea improved significantly and swelling and inflammation of her lower limbs decreased. The follow-up CXR also showed a decrease in cardiac index (compared with the previous abnormal size (Figure 3). In follow up echocardiography, PAP just decreased 10 mmHg to reach the level of 70mmHg and TR++ was noted. Other indices showed no significant changes. Swelling and erythema of the left breast which was due to superficial phlebitis resolved by the treatments mentioned above. DISCUSSIONBehcet’s disease is accompanied by disturbances in different organs, with 25-35% of cases showing vascular complications.1 These complications, increase morbidity and mortality of the disease and worsen the prog-nosis.2 On the other hand, like other vasculitides, we don’t have a curative treatment for it. In this disease, vascular complications are in three forms: 1) Systemic arterial vasculitis These vascular complications are due to obstruction in venous and arterial flow, aneurysmal formation and varices.2 Significant differences in vascular involvement are observed among patients from different parts of the world, for instance, venous complications are more commonly observed in Turkish and Iranian cases while in Japanease cases, arterial complications are more com-mon.2,3 In an Iranian report by Naji et al, vascular complications were observed in 349 out of 3737 cases (8.5%); from those, 228 cases suffered from DVT of limbs, 86 cases had superficial venous thrombosis and 37 cases had visceral and large vein thrombosis. Arterial complications were observed in 16 cases (0.4%), among them 12 cases had arterial aneurysms, 1 case had arterial thrombosis and 3 cases had decrease arterial pulses.4 The remarkable point about our case is that hemoptysis can occur due to DVT and pulmonary emboli or pulmonary artery vasculitis. It goes without saying that the differential diagnosis between pulmonary emboli and pulmonary artery vasculitis (as the cause of hemoptysis) can be life saving to the patient, as pulmory emboli are treated with heparin and warfarin while this treatment can lead to severe and life threatening hemoptysis if pulmonary vasculitis happens to be the cause. On the other hand, a patient with vascular complications can have arterial and venous complications at the same time. It means that the patient might have deep vein thrombosis of legs leading to pulmonary emboli and hemoptysis, but he/she has pulmonary artery vasculitis, too. It should be mentioned that in Behcet’s disease, detachment of thrombotic clot in leg veins are not common but the patient has pulmonary thromboemboli with calf vein origin.5 Angiography and MR angiography (if available) can help us in differential diagnosis and confirm pulmonary vasculitis in these cases.6 Before admission in our center and with the suspicion of pulmonary emboli, the discussed case was treated with heparin and as the hemoptysis didn’t worsen, the therapy continued and pulmonary angiography requested (to be done electively) and afterwards the clinical picture improved significantly. REFERENCES
Copyright 2004 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr04032f3.jpg] [mr04032f1.jpg] [mr04032f2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}