 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
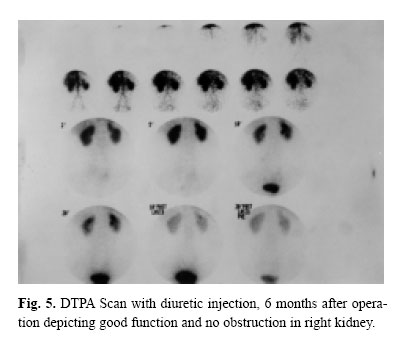
Medical Journal of the Islamic Republic of Iran , Vol. 18, No. 2, August, 2004, pp. 177-180 THE APPENDIX, AN ACCEPTABLE SUBSTITUTE FOR ALL SEGMENTS OF BOTH URETERS: A REPORT OF TWO CASES M.A. ZARGAR M.D., M. MIRZAZADEH, M.D.*, AND K. ZARGAR From the Dept. of Urology, Hashemi Nejad Hospital, Iran University of Medical Sciences, Tehran, I.R. Iran. Email : mjmirza@iums.ac.ir-Tel.0912-1256222. Code Number: mr04033 ABSTRACTThere are occasional reports of using the appendix to replace sections of the ureters, and to our knowledge, only a couple of them were in the left side. We used the appendix as a ureteral substitute in two cases in technically difficult parts, the upper left ureter and the first part of the right ureter. Follow-ups of 8 years and 6 months in right and left side cases, respectively, are impressive with maintenance of patency and improving renal function. We believe that the use of the appendix is a valuable alternative to substitute all segments of both ureters, with good results. Keywords: Ureter, Injury, Replacement, Appendix Vermicularis. INTRODUCTIONRepairing long ureteral injuries especially in the upper segments, is challenging. There are multiple, yet suboptimal solutions including: ureterocalycostomy, renal descensus, autotransplantation of the kidney to the iliac fossa, permanent nephrostomy tube drainage, ileal interposition, and use of the appendix vermicularis.1,2 Use of the appendix as a ureteral substitute began in 1912 by Melinkoff,3 but it did not become a popular method at that time. There are other reports of using the appendix as a right ureteral substitute. A recent article reports good long term results of using the appendix to replace the right ureter in three children.8 We report two cases of using the appendix to substitute the first part of the right ureter and the upper part of the left ureter. CASE REPORT Case 1 A 23 year old man was referred to us in 1994, who had a right side nephrostomy tube for six years. He had a history of several operations on his kidneys. At the age of 5 he had undergone ureterolithotomy for the left upper ureteral stones; at the age of 11, bilateral pyelolithotomy for renal pelvis stones, and at the age of 17, bilateral open pyeloplasty to repair UPJO (ureteropelvic junction obstruction) had been done. Two months after UPJO repair, the patient became more symptomatic, therefore a nephrostomy tube was inserted (1988). Since then the patient has had a nephrostomy tube in the right kidney. When he was referred to us, he described vague pain in both flanks and symptoms of recurrent urinary infections. His serum BUN and creatinine were 28 mg/dL and 1.4mg/dL respectively (normal range were up to 20, and up to 1.2, respectively). In antegrade and retrograde evaluation, there was a relatively long defect between the right pelvis and upper ureter. Technique After bowel preparation, and with a midline transperitoneal incision, the right kidney, pelvis and upper ureter were exposed. We decided to use the appendix due to adhesions of three previous operations. We separated the base of the appendix from the cecum and excised its tip. The appendix with its vascular pedicle (one of the end branches of the ileocecal artery) was transferred to the upper ureter fossa. After irrigation of the lumen and spatulating of both ends, we anastomosed the base of the appendix to the pelvis and the tip to the upper ureter with a single layer of 4-0 chromic catgut sutures on a previously inserted stent. Afterwards we covered all around the anastomosis with a portion of omentum, and a new nephrostomy tube was inserted through the old rephrostomy tract. Four weeks later, the stent was removed and after one week antegrade pyelography showed good passage of dye through the ureter down to the bladder. Therefore the nephrostomy tube was clamped and subsequently removed with no leakage. We performed an IVU one month later, which showed good excretion and passage of dye. Currently more than 8 years after the operation our patient is asymptomatic, with no urinary infections. And his serum BUN and creatinine are 8.1 mg/dL and 1.2mg/dL respectively. A 37 year old woman was referred to us in March 2000, because of fever, chills and left flank pain. In past history she had shockwave lithotripsy 6 months previously due to left kidney stones. Subsequently, the patient had undergone transureteral lithotripsy (TUL), due to impacted fragments of stone in the left upper ureter, and because of suspected ureteral injury during TUL, the patient had an emergency operation to remove the stones and to repair the ureter with insertion of a stent. After removing the JJ stent 2 months later, she was referred to us because of fever, chills and left flank pain. In our evaluations, with IVU (intravenous urography) the left kidney was faintly visualized. Attempts of retrograde catheterization of the left ureter were unsuccessful, because of previous manipulations. Therefore a percutaneous nephrostomy tube was inserted and antegrade pyelography was performed. There was complete obstruction of the ureter about 5 cm below the the left UPJ. As the general condition of the patient improved, she was operated on. During the operation we explored the left ureter. There was a fibrotic stenosis at the previously operated portion of the left upper ureter measuring more than 6 cm. After considering our options, we decided to use the appendix. Therefore we transferred the appendix with right colon and distal ileum to the left upper ureteral fossa, and anastomosed the spatulated base of the appendix to the upper segment and spatulated the tip to the lower segment of ureter on a JJ stent (the technique was identical to that of the previous patient). We removed the JJ stent 6 weeks later, and the patient was free of symptoms thereafter. IVU 6 months after operation showed great improvement of function and little hydronephrosis. Radionuclide scan showed good function with no obstruction in the left side. DISCUSSIONUreteral injuries are not common, but with more frequent use of ureteroscopy, the incidence of such injuries are increasing rapidly. There are several, yet suboptimal ways to repair such ureteral defects. The results of using the appendix as a ureteral substitution (although almost all reported cases involve the right side) are en-couraging.7,8,9 The appendix has an irregular lumen, approximately 8 Fr. in diameter. The blood supply arises from the appendicular artery, a branch of the ileocolic artery located in the mesoappendix.13 Histologically, the appendiceal muscle wall has a circular orientation, and its peristalsis is from the base to the tip.3 There are many advantages in using the appendix as a ureteral substitute; good contractility, the ability to be mobilized with its blood supply to reach any part of both ureters, no need for bowel anastomosis, negligible urine absorption, the possibility of creating a submucosal tunnel to prevent reflux in lower ureteral cases, and correspondence of appendiceal caliber to that of the ureteral lumen.5,11 Limitations to use of the appendix include inadequate length (sometimes only 2 cms), previous inflammation or appendectomy.12 Two important technical points in using the appendix are: base to tip direction of peristalsis in the appendix, so the base should be anastomosed to the proximal and the tip to the distal part of the ureter, and the necessity of adequate mobilization to achieve a tension-free anastomosis to the right or left ureter.5,13 Regarding the suboptimal results of all other procedures to substitute long segments of ureter and the impressive results of our patients in the most difficult parts of ureters to be substituted, in two very difficult cases with multiple previous operations, we consider ureteral replacement with the appendix as an acceptable option. We therefore believe that the appendix is a valuable substitute for all portions of both ureters with encouraging results. Due to the increasing rate of ureteral injuries , a prospective study to determine the long term results of using the appendix comparing to other alternatives is necessary. REFERENCES
Copyright 2004 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr04033f1.jpg] [mr04033f3.jpg] [mr04033f5.jpg] [mr04033f2.jpg] [mr04033f4.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}