 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
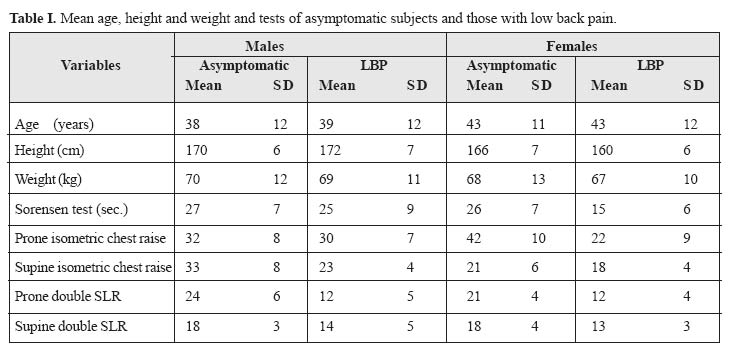
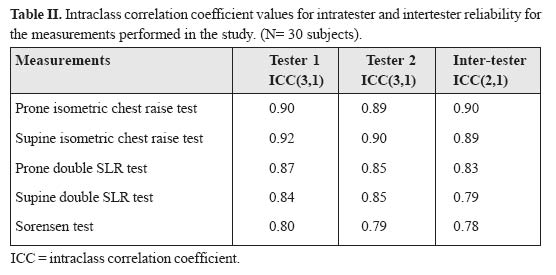
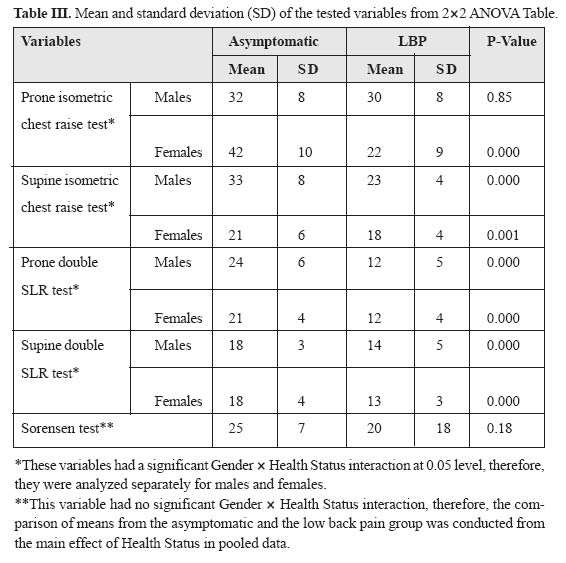
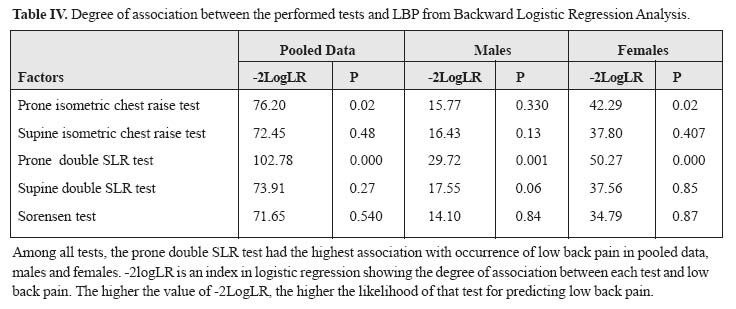
Medical Journal of the Islamic Republic of Iran , Vol. 19, No. 2, August, 2005, pp. 95-101 CLINICAL TRUNK MUSCLE ENDURANCE TESTS IN SUBJECTS WITH AND WITHOUT LOW BACK PAIN ISMAEIL EBRAHIMI, PT., Ph.D., GHOLAM REZA SHAH HOSSEINI,M.D., MAHYAR SALAVATI, PT., Ph.D., HOSSEIN FARAHINI, M.D.,AND AMIR MASSOUD ARAB, PT., M.Sc. From the University of Social Welfare and Rehabilitation Sciences, Tehran, and Iran University of Medical Sciences, Tehran, Iran. Corresponding author: Amir Massoud Arab, PT., M.Sc., Shahrak Telephone: (++98) 21 88096329, Fax: (++98) 21 22418764 Gharb, Hormozan Street, Soroush Alley, No:10, Tehran 14667, Iran, E-mail: arabloo_masoud@hotmail.com Code Number: mr05001 ABSTRACT Study design: A cross-sectional non-experimental study. Keywords: Muscle endurance, Low back pain, Test. INTRODUCTIONLow back pain (LBP) is one of the most common complaints in today’s societies.1 Some studies have indicated that about 70-80% of the population have had at least one episode of LBP in their life-time.1 Several factors, based on assumptions, clinical findings and scientific experiments, have been associated with the development of LBP. However, during the past decades the main focus has been placed on back muscle endurance and its association with LBP. Back extensor muscles are postural muscles that aid in maintaining the upright standing posture and controlling lumbar forward bending.2 Several studies have reported a significant decrease in back extensor muscle endurance in patients with LBP.2,3,4,5 It is thought that decreased back muscle endurance causes muscular fatigue and overloads soft tissue and passive structures of the lumbar spine, resulting in LBP.6,7 Biering-Sorensen8 has identified poor back extensor muscle endurance as an important risk factor for LBP. Others have suggested that a test of back extensor endurance be used as a screening tool in the selection of workers for strenuous jobs. Since trunk extensors are classified as postural muscles,9 they are rich in larger diameter type I muscle fibers and are suited to support low levels of activity for long periods of time.10 Moreover, electromyographic (EMG) studies indicate that the paraspinal muscles in patients with LBP have a faster fatigue rate compared with those in asymptomatic subjects11,12,13 that indicate the significance of these muscles in occurrence of LBP. Hides et al14 showed a 31% decreased cross-sectional area in lumbar multifidus muscles in patients with LBP, which did not resolve automatically after remission of the painful symptoms. According to Roy et al,5 these muscles consistently demonstrate a higher fatigue rate in patients with LBP. Furthermore, besides the endurance of back extensor muscles some investigators have focused on the endurance of the trunk flexors in LBP because of their significant role in normal function of the lumbo-pelvic area. Ito et al.16 have shown a significant decrease in trunk flexor endurance in patients with LBP. As noted above, most previous studies have shown the significance of muscle endurance in LBP. So testing spinal muscle endurance seems very important in prediction, prevention and rehabilitation of LBP. Several types of methods of testing such as static endurance test, active measures of endurance, isokinetic and EMG testing have been studied in the literature.17 From these assessment strategies, isometric endurance testing seems to be cost-effective and require little equipment for doing in the clinics. Because of these features, investigators have focused mainly on isometric endurance assessment. They believed that it would be the type of testing that clinicians would choose to use to measure spinal muscle endurance. Different static endurance testing methods and evidence regarding their utilization have been reported in the literature. Most commonly, these are: prone isometric chest raise test as described by Ito et al16 and McIntosh et al,18 prone double straight-leg raise test as described by McIntosh et al,18 supine isometric chest raise test as described by Ito et al,16 supine double straight-leg raise as described by Kendal19 and Sorensens8,20,21 test. Although several studies have shown a significant difference between normal subjects and those with LBP in these tests, more in-depth review of these articles reveals that most previous studies have considered only one of these tests in a relatively small population. Furthermore, although these tests have been used to measure endurance of the muscles, identification of tests with more dominant sensitivity on assessment of LBP has not yet been accomplished. The aim of this study was to detect the reliability and feasibility of the five types of clinical examinations in subjects with and without LBP in a relatively large population and to identify the sensitivity of each test to predict the probability of the occurrence of LBP. PATIENTS AND METHODS Subjects A total of 200 subjects between the ages of 20 and 65 were randomly selected from four hospitals in Tehran, Iran. Subjects were categorized into four groups: asymptomatic males (N= 50, mean age= 38+12 years), asymptomatic females (N= 50, mean age = 43(11 years), males with LBP (N= 50, mean age= 39+12 years), and females with LBP (N= 50, mean age = 43+12 years). To account for the effect of age on the considered tests, the subjects in each category were matched by age. The mean age, height and weight of the subjects in each group are shown in Table I. Selection criteria Subjects were included if they had no history of spinal surgery, no spinal or pelvic fracture, no history of hospitalization for severe trauma or injuries from a car accident, no history of osteoarthritis or fracture of the lower extremities and had no history of any systemic disease, such as arthritis or tuberculosis. Asymptomatic subjects were evaluated and found to have no complaint of any pain or dysfunction in their low back, thoracic and neck area and lower extremities. Patients were included if they had a history of LBP for more than six weeks before the study or had on and off back pain and had experienced at least three episodes of LBP, each lasting more than one week, during the year before the study. None of the subjects with or without LBP had referred leg pain. Before participating in the study, all subjects signed an informed consent form approved by the human subjects committee of the University of Social Welfare and Rehabilitation Sciences. Reliability assessmentThe inter-tester reliability of the measurements were assessed in 30 asymptomatic subjects (15 male and 15 female volunteers). The first examiner completed the tests in a subject and then after 15 minutes repeated the tests in a random order on the same subject. The second examiner, then, tested the subject, following the same procedure. ProceduresFive types of clinical physical examination for estimation of the endurance of spinal muscles were used in this study. The description of the procedure and the instruments used to measure each variable are as follows. Sorensen testThe Sorensen test is the method most frequently investigated and reported in the literature.8,17,20,21 BieringSorensen8 described this method of testing isometric back endurance. It measures how long (to a maximum of 240 seconds) the subject can keep the unsupported trunk (from the upper border of the iliac crest) horizontal while prone on an examination table. During the test, the buttocks and legs are fixed to the table by three wide canvas straps and the arms are folded across the chests. The subject is asked to maintain the horizontal position until he/she can no longer control the posture or has no more tolerance for the procedure. Prone isometric chest raiseThis test was done with the subject lying prone on a treatment table with the hands laying beside his/her trunk. A small pillow was placed under the lower abdomen to decrease the lumbar lordosis. The subject was instructed to lift the upper trunk exactly 30° from the table and hold the sternum off the floor for as long as possible. The detailed procedure for this test is described by Ito et al.16 and Moreau et al.17 Prone double straight-leg raiseFor the prone double straight-leg raise, the subjects lay in a prone position, hips are extended, with the hands underneath the forehead and the arms rested perpendicular to the body. The subject was then instructed to raise both legs until knee clearance was achieved. The examiner monitored knee clearance by sliding one hand under the thighs. The time was recorded in seconds, and the test was terminated when the subject was no longer able to maintain knee clearance. The detailed procedure for this test is described by Mc Intosh et al.17,18 Supine isometric chest raiseThis test was done with the subject lying supine on a treatment table with the hands crossed on his/her chest. The knees and hips were in 90° flexion. The subject was instructed to lift his neck and upper trunk from the table and hold this position for as long as possible. The detailed procedure for this test is described by Ito et al.16 Supine double straight-leg raiseFor the supine double straight-leg raise, we followed the method described by Kendall et al19 to assess the endurance of lower abdominal muscles. The subject began in the supine-lying position, hips extended, with the hands laying beside his/her trunk. The subject was then instructed to raise both legs from the floor about 20 degrees and hold this position for as long as possible without any tilting in the pelvis. The examiner monitored pelvic tilt during the test. The time was recorded in seconds and the test was terminated when the subject was no longer able to maintain knee clearance. Data analysisWe used intra-class correlation coefficient (ICC), two way random effect model22 to assess inter-tester and intra-tester reliability of the measurements. We tested quantitative data by using 2*2 ANOVA, accounting for gender, health status (symptomatic vs. asymptomatic), and interaction of health status and gender effects. We used pooled data where there was no significant health by gender interaction effect, but analyzed the data separately for males and females for the variables which had a significant health status by gender interaction. To determine the relative sensitivity of each test on likelihood of LBP occurrence, the tests which were found significantly different between subjects with and without LBP were selected and backward logistic regression analysis was used to determine the effect of each test on the probability (likelihood) of LBP occurrence. Logistic regression analysis is a statistical procedure used to predict the probability of the occurrence of a dichotomous dependent variable as a function of the independent variables.69 RESULTSTable II presents the ICC for each test taken in the pilot study. Except for the Sorensen test and supine double SLR test, all other ICC values were greater than 0.80 (Table II). The result of 2*2 ANOVA revealed that gender by health status was significant for prone isometric chest raise, prone double straight-leg raise, supine isometric chest raise and supine double straight-leg raise tests at α= 0.05. Therefore, these factors were analyzed separately for males and females. We found that prone double straight-leg raise, supine isometric chest raise and supine double straight-leg raise tests were significantly different between normal males and females and those with LBP. For prone isometric chest raise, a significant difference was found only in females with and without LBP but not in males (Table III). We used pooled data to compare means of the Sorensen test, which had no significant health status by gender interaction effect, across subjects with and without LBP. The result showed that Sorensen test was not significantly different between normal subjects and those with LBP (Table III). We used backward logistic regression analysis to determine the association between LBP and performed tests. In pooled data, among all the tested variables, prone double straight-leg raise test had the highest as sociation with occurrence of LBP (Table IV). Other tests remained in the model but were not highly associated with LBP (Table IV). In separate analysis of data for males and females (Table IV), prone double straight-leg raise test also showed the highest association with LBP. DISCUSSION Our data indicate that a significant difference in all performed tests exists between subjects with and with out LBP. This finding is in accordance with other studies showing a significant decrease in trunk muscle endurance in patients with chronic LBP.2,3,4,5 The importance of this factor has been emphasized in the literature. Investigators have identified poor back extensor muscle endurance as an important risk factor for LBP. Because these muscles are rich in larger diameter type I muscle fibers,23 they are suited to support low levels of activity for long periods of time.10 Electromyographic (EMG) studies, however, indicate that the paraspinal muscles in patients with LBP have a faster fatigue rate compared with those in asymptomatic subjects.11,12,13 Investigators have attributed the decreased muscle endurance found in patients with LBP to higher muscle metabolite level resulting from prolonged muscle tension and spasm,24 muscle deconditioning13 and inhibition of the paraspinal muscles13 in response to pain and decreased activity. The significant difference in performed tests between subjects with and without LBP found in our study complements the results of previous studies which indicated that improvement of muscle endurance is an important factor in preventing8 and treating25 LBP. However, the significance of this study is due to assessing several tests have been used to measure endurance of the muscles together to compare the relative significance of each test to identify which test has greater sensitivity for assessment of LBP. Our data indicate that among all clinical tests to assess the endurance of trunk muscles, prone double straight-leg raise has the highest association with LBP comparing with others. McIntosh et al.18 state that this test assesses the lower back extensor muscles while others such as prone isometric chest raise, Sorensen and supine isometric chest raise assess upper back extensor and flexor endurance. Perhaps the high association with prone double straight-leg raise test with LBP found in our study is due the fact that inhibition and atrophy of the lower paraspinal muscles13 especially the lumbar multifidus muscles,26,27 is very important in causing LBP because of muscle deconditioning,13 impaired muscle coordination and unequal distribution of muscle force . Hides et al.14 showed a 31% decreased cross-sectional area in lumbar multifidus muscles in patients with LBP, which did not resolve automatically after remission of painful symptoms. According to Roy et al,5 these muscles consistently demonstrate a higher fatigue rate in patients with LBP. Our data showed no strong association between LBP and the Sorensen test. Although the Sorensen test is the method frequently investigated and reported in the literature, controversy exists as to the amount of endurance that is provided by the lower lumbar extensors in contrast with the hip extensor which contributes to the performance of the test. Moffroid et al25 found a significant positive correlation between EMG median frequency slopes of the biceps femoris and Sorensen test results. They conclude that the Sorensen test fatigues the biceps femoris more than the lower erector spinae and that it indicates more about the endurance of the hip extensors than that of trunk extensors. Another issue that should be considered in clinical use of the Sorensen test procedure is its difficulty. Previous studies reported subjects have difficulty during the Sorensen test. In Biering-Sorensen’s study, 24% of the sample could not complete the test, primarily due to back pain followed by pain in the legs or abdomen. Latika et al28 also reported a 50% failure rate in doing the Sorensen test. REFERENCES
Copyright 2005 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr05001t3.jpg] [mr05001t1.jpg] [mr05001t4.jpg] [mr05001t2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}