 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Medical Journal of the Islamic Republic of Iran , Vol. 19, No. 2, August, 2005, pp. 119-125 COMPARISION OF THE EFFICACY OF NEBULIZED L-EPINEPHRINE, SALBUTAMOL AND NORMAL SALINE IN ACUTE BRONCHIOLITIS:A RANDOMIZED CLINICAL TRIAL J. KHASHABI, S. SALARI LAK, M. KARAMIYAR, AND H. MUSSAVI From the Department of Pediatrics, Imam Medical Center, Urumieh University of Medical Sciences, Urumieh, I.R. Iran. Correspondence: Javad Khashabi, M.D., professor, Department of Pediatrics, Imam Medical Center, University of Medical Sciences, I.R. Iran. Email: jkhashabi@umsu.ac.ir, Tel: +984413444544, Fax: +984413445939 Code Number: mr05004 ABSTRACTBackground: Acute bronchiolitis is the most common form of lower respiratory
tract infection in infancy. There are numerous contradictory reports regarding
the efficacy of nebulized bronchodilators in the management of infants with
acute bronchiolitis. This study was designed to compare the efficacy of nebulized
epinephrine with salbutamol for treatment of the disease. Keywords: Epinephrine, Salbutamol, Bronchiolitis, Clinical trials, Infants. INTRODUCTION The clinical syndrome of acute bronchiolitis is the most common form of lower respiratory tract infection in infancy. It is an extremely common problem in children less than two years of age with a reported attack rate in The clinical syndrome of acute bronchiolitis is the the Western literature being as high as 11.4 percent of most common form of lower respiratory tract infection in children in the first year and 6 percent of children in the second year of life.1 Approximately 1 percent of healthy infants are hospitalized with this infection annually and 8% of hospitalized children will require intensive care.1,2,3 Bronchiolitis is predominantly a viral illness. The respi-
Table II. Demographic characteristics of patients in the study groups.
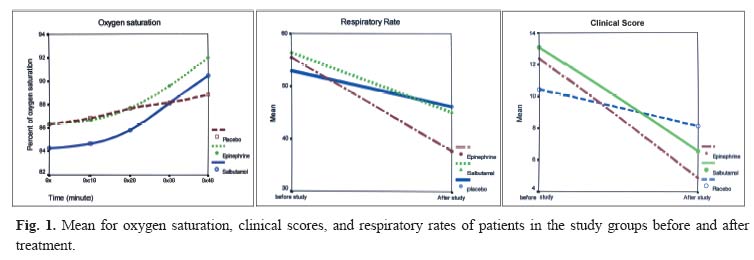
ratory syncytial virus (RSV) is the causative agent in more than 50% of cases.1,4 Viral respiratory tract infections in infants are often associated with small airway obstruction secondary to an inflammatory process and / or spasm of the bronchial musculature and accumulation of mucus and cellular debris. It is difficult to make an exact diagnosis in the absence of the facilities for the viral culture and pathological findings, therefore usually a clinical diagnosis of bronchiolitis is made.1,4,5 Careful monitoring and good supportive care remain the cornerstones of management. All pediatric textbooks recommended hospitalization of patients and providing cool humidified oxygen to relieve hypoxemia and reduce insensible water loss from tachypnea.5,6 One of the biggest contentions in the management of acute bronchiolitis is the role of bronchodilators. Some authorities frequently argue that there is little doubt regarding the effectiveness of bronchodilators and these agents are used extensively.2,7 On the other hand several studies have failed to show any benefit from the use of β2-agonists.3,8,9 It is hypothesized that alpha-agonists might provide effective relief of airway obstruction caused by mucosal edema.1,10 Epinephrine has a number of advantages over β2adrenergic selective bronchodilators that ensure its efficacy with fewer side effects. Epinephrine increases airway caliber through bronchodilation by β2 sympathomimetic activity, reversal of tissue edema through vasoconstriction by α1 actions, and physiological antihistamine effect, which ensures mucosal decongestion. Most studies reported some improvement in short-term outcomes, although the Table III. Comparison of initial and final parameters in the study groups and between them.
condition of a few patients worsened.1,7,11 Traditionally racemic epinephrine has been used, as a nonselective adrenergic agonist of choice in infants with bronchiolitis due to its supposedly fewer side effects than the more active and more readily available natural laboratory form of epinephrine. However there seems to be no pharmacological basis for this data.1,12 In addition, L-epinephrine is readily available, while racemic epinephrine is not available in countries like Iran. We conducted a randomized, double blind, placebo controlled study to examine the efficacy of nebulized epinephrine, salbutamol and normal saline (as a placebo) on clinical scores and oxygenation of patients admitted in an emergency department. The aims of this study were to evaluate the safety and the clinical responses to nebulized L-epinephrine and salbutamol in infants with acute bronchiolitis. MATERIAL AND METHODSThis study was a prospective double-blind randomized placebo-controlled clinical trial, approved by the research and ethic committee of Urumieh Medical School. This study was conducted in infants (2-24 months old) with a clinical diagnosis of viral bronchiolitis referring to the pediatric emergency department of Imam hospital, a tertiary medical care facility in Urumieh, Iran, from October 2002 till May 2003. Clinically viral bronchiolitis was defined as an acute viral infection of the lower respiratory tract, preceded or accompanied by fever and/or rhinitis and characterized by tachypnea, expiratory wheezing, and increased respiratory effort. Infants with previous history of wheezing or bronchodilator therapy before current illness or underlying chronic cardiac, pulmonary disease and bronchopulmonary dysplasia were excluded from the study. Patients were evaluated for enrollment by one of the study investigators (M.H.) using a standardized complete respiratory history including age, gender, duration of illness, history of previous wheezing, current medication, allergies, family history of asthma, chronic illness and cardiac or pulmonary diseases. Other causes of acute wheezing in infancy like foreign bodies were evaluated and ruled out. The severity of illness was assessed clinically (clinical score) by using a modified combination of RDAI score (respiratory distress assessment index) and Yale1,7 observation scale (Table I). These two scores are the most frequently used by clinicians which are non-invasive and have a good interobserver agreement. Patients were divided into mild, moderate and severe disease, based on the sum of the clinical scores. Children with total scores of 0-8, 9-18 and >19 were classified as having mild, moderate, and severe disease respectively. All eligible patients with moderate disease were included in the study. Patients with mild and severe disease were excluded from the study and those with severe bronchiolitis were admitted in the hospital. Patients were randomly assigned to receive either epinephrine, (Daroo-Pakhsh Tehran, Iran) 0.1 mL /kg body weight of 1 in 10000 solution, salbutamol ( Ventolin,Glaxo Wellcom Australia Ltd Boronia, Australia) 0.15 mg/ kg body weight or normal saline as a placebo. The drugs were mixed with normal saline to make a total volume of 5 mL and were nebulized (Soniclizer 305 ATOM Medical Corp Tokyo, Japan) with oxygen flow of 8 liter / min. All solutions were identically clear and similar in appearance. All study personnel and participants were unaware of the treatment assignment. Three doses of each drug were given at 20-minute intervals. Oxygen saturation values were recorded at the start of the study and ten minutes after the first, second and third doses of the drug. Oxygen saturation (SaO2) was measured noninvasively by using pulse oxymetry. No other drugs like antibiotics or steroids were administered during these periods. The infants were assessed before and 10 minutes after each treatment. Ten minutes after administration of the last dose of the study drugs, the clinical respiratory distress assessment score was evaluated again to determine the response of therapy . The decision for further management was taken on the basis of this evaluation. Children who showed a sustained decrease in tachypnea and respiratory distress and tolerated oral feeding, were sent home after an observation period of three hours on oral medication. Children who did not improve or showed deterioration were admitted in the hospital for further management. Acute bronchiolitis was the final diagnosis in these admitted patients. Sample sizeThe study was designed to detect a difference of at least 5% in SaO2 (mean level of oxygen saturation) and total clinical score between the 3 drugs with alpha (two tailed) of 0.1 and Power (1-b) of 0.90. The standard deviation for this calculation was taken as 4 as determined from the pilot study. This gave a sample size of 24 in each arm of the study. RESULTSA total of 72 infants with moderately severe bronchiolitis were enrolled in three equal groups. There was no significant difference between the groups at randomization in terms of demographic variables (Table II). The mean age of the children was 9.1 months. The mean initial clinical scores, respiratory rates, and the minimum levels of SaO2 did not show significant difference the between the study groups. After nebulization the various study parameters such as respiratory rate, SaO2, and clinical score were compared with initial values (Table III, Fig. 1). At the end of the study, the mean SaO2 rose from 86.4 to 91.9 in epinephrine and 84.3 to 90.5 in salbutamol groups and showed significant differences between pre-and post- interventions (p= 0.00). There was no similar difference in the placebo group (SaO2 raised from 86.3 to 88.8, (p= 0.1). Oxygen saturations recorded after the third dose of nebulization, showed significant improvement in all study groups, but in the epinephrine group mean oxygen saturation was significantly higher than salbutamol and placebo groups (p= 0.04). Comparison of respiratory rates in the 3 study groups showed that there were significant differences in the pre-and post-study results (p= 0.00), but in the epinephrine group results were better than other groups (t: 11.0). Pre- and post-interventional respiratory distress assessment scores (clinical score) showed significant differences in all the study groups (p= 0.035). Improvement in epinephrine and salbutamol groups was better than the placebo group. At the end of the study 16 out of 24 patients in the epinephrine group (66%), 12 out of 24 children in the salbutamol group (50%), and only 6 out of 24 patients in the placebo group (25%) showed significant improvement to a degree that they could be sent home. Initial and final parameters of the study groups and between them are presented in Figure 1 and Table III. There were no serious adverse clinical side effects of the drugs like increased irritability, tremors, facial blanching, congestive heart failure, tachycardia and arrhythmia during the study. DISCUSSIONBronchiolitis is an extremely common problem in children less than two years of age and is the most frequent cause of hospitalization for respiratory infection in early childhood.6,13 The main objective of the clinician is to provide long lasting relief from respiratory distress by decreasing wheezing and improving air entry.2,5,6 The treatment is largely supportive. Viral respiratory tract infection in infants is often associated with small airway obstruction secondary to an inflammatory process and / or spasm of the bronchial muscular tone. Bronchodilators are widely used in many countries for infants with bronchiolitis. In Canada 68-96 percent of infants with bronchiolitis are treated with bronchodilators.14 In another study 54 of 88 European pediatric centers reported using bronchodilators in all patients with bronchiolitis, and 15 centers reported using bronchodilators only in high-risk patients.15 It is hypothesized that the alpha and beta agonist agents such as epinephrine and salbutamol may improve the clinical signs and symptoms of patients by relieving pathological changes of the disease.1,2,5,6 Since then, numerous adrenergic agonists, specific and non-specific, like salbutamol, racemic epinephrine, etc., have been used in the nebulized form with different results.1,3,16,17,18 Controversy still remains about the nature, route and dosage of the drugs to be used.19, 20,21,22 The present study has attempted to verify the efficacy of bronchodilators in bronchiolitis and compare the benefits of adrenergic specific and non-specific agonists with a placebo among children presenting with a first episode of wheezing and respiratory distress in association with fever and / or coryza, without any family history of atopy or asthma. After nebulization of three doses of the study drugs, both epinephrine and salbutamol groups showed significant improvement in mean respiratory rate, clinical scores and SaO2 in comparison with the placebo group that mildly improved in various parameters. However these changes were significantly marked in the epinephrine group in comparison to the salbutamol group for clinical scores and respiratory rate. Some investigators cite the advantage of racemic epinephrine in the treatment of bronchiolitis, and some reports indicate that L-epinephrine is well tolerated too.1,11 Menon et al.20 also noted that infants receiving nebulized epinephrine had a significantly lower heart rate than did a similar group receiving nebulized salbutamol. Many trials of bronchodilators in bronchiolitis have been reported; some of them compared epinephrine with salbutamol, while others compared epinephrine or salbutamol with placebo. But there are a few reports to compare the efficacy of salbutamol, epinephrine with placebo together. To test whether nebulized salbutamol is safe and efficacious for the treatment of young children with acute bronchiolitis, Klasen and collegues19 enrolled 83 children in a randomized double - blind clinical trial. They conclude that salbutamol is safe and effective for the initial treatment of young infants with bronchiolitis. In another study the efficacy of nebulized salbutamol was compared against normal saline. Patients in the salbutamol group exhibited significantly greater improvement in respiratory rate and clinical score.23 In some studies the results of nebulized salbutamol in the treatment of acute bronchiolitis were not satisfactory. Dobson24 et al. in a clinical trial compared the efficacy of nebulized salbutamol and normal saline in hospitalized infants with bronchiolitis. They concluded that the treatment does not appear to enhance recovery or attenuate severity of illness. In another study a randomized clinical trial was conducted on young children with moderate bronchiolitis. There was no role for nebulized sulbutamol and ipratropium, either as a single agent or in combination, compared with normal saline in treating young children in hospital with bronchiolitis.3 Flores and Horwitz25 in a critical review and meta-analysis of randomized controlled trials evaluated the efficacy of β2 agonist in bronchiolitis. The authors reviewed three inpatient and five outpatient studies. They concluded that the evidence for the efficacy of β2-agonists therapy for bronchiolitis remains unavailable. There are many studies about the use of epinephrine in brochiolitis. In a multicenter, randomized, double blind, controlled trial the effect of nebulized epinephrine was examined on the length of hospital stay. The use of nebulized epinephrine did not significantly reduce the length of hospital stay.26 In another meta-analyzed study of randomized controlled trials Hartling et al.27evaluated the efficacy of epinephrine for the treatment of acute viral bronchiolitis. They concluded that epinephrine might be favorable compared with placebo and salbutamol for short-term benefits among outpatients. There was insufficient evidence to support the use of epinephrine among inpatients. The authors recommended large, multi-centered trials before routine use of the drug among outpatients. To investigate whether nebulized racemic epinephrine or salbutamol improves respiratory distress in infants with acute bronchiolitis, Reijonen and colleagues17 conducted a double - blind randomized, placebo controlled study. A comparison of paired data of each patient revealed that the difference in variables were significant between racemic epinephrine and saline, but not between salbutamol and saline. In another clinical trial, 91 infants with their 1st or 2nd episode of wheezing associated respiratory tract infection were enrolled in the study. The authors concluded that both L - adrenaline and salbutamol caused significant improvement in mean symptom score and oxygenation. However the adrenaline group showed a significantly better improvement in the study parameters than the salbutamol group.1 And finally Mull et al.28 in a randomized trial concluded although the patients treated with epinephrine were judged well enough for discharge significantly earlier than the patients treated with albuterol, epinephrine was not found to be more efficacious than albuterol in treating moderately ill infants with bronchiolitis. In our study nebulization of normal saline as a placebo had beneficial effects on clinical scores and oxygen saturation. It is thought that saline produces its effects by liquefying dry secretions, assisting their clearance, and by humidifying and soothing injured mucosal surfaces, hence reducing irritation.13 In summary in this study all treatment groups demonstrated clear evidence of clinical improvement and oxygen saturation, but epinephrine and salbutamol in comparison with placebo showed more efficacy in relieving symptoms and improving oxygenation in infants with acute bronchiolitis. Finally L-epinephrine demonstrated better efficacy in relieving respiratory distress and improving oxygen saturation as well as decreasing the need for hospitalization than salbutamol. On the results of this study we recommend nebulized L-epinephrine for treatment of out-patient infants with moderately severe acute bronchiolitis. ACKNOWLEDGEMENTWe would like to thank Prof. Farrokh Ghavam for his guidelines and the nursing staff of the Pediatric Dept. of Imam hospital (Urumieh, Iran) for their kind cooperation in conducting this study. REFERENCES
Copyright 2005 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr05004f1.jpg] |
| |||||||||
{kind=link}