 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Medical Journal of the Islamic Republic of Iran , Vol. 19, No. 2, August, 2005, pp. 147-151 CHARACTERISTICS AND PREVALENCE OF OCCULT HEPATITIS B VIRUS INFECTION IN PATIENTS WITH HEPATITIS C IN IRAN TAHEREH ZANDIEH *, NADER COHAN, SHAHRAM SAMIEI,SEDIEGHEH AMINI, ZAHRAATAEI, AND MAHNAZ KAVARI From the Research Center of the Iranian Blood Transfusion Organization, Tehran, Iran. *Scientific Member & Assistant Professor of IBTO, Iranian Blood Transfusion Organization, Sheikh Fazlollah Expressway, Shahid Hemmat, Tehran, Iran. Fax: 00 98 21 88601518, Tel: 88288581-3 E-mail:zandyeh@ibto.ir rnegative Code Number: mr05009 ABSTRACTBackground: Hepatitis B virus (HBV) infection in patients who lack detectable hepatitis B surface antigen (HBsAg) is called occult hepatitis B infection. Such infections have been frequently identified in patients with chronic hepatitis C liver disease, but their prevalence is not known. Keywords: Occult hepatitis B, Surface antigen, chronic hepatitis C, PCR. INTRODUCTION Hepatitis B virus (HBV) and hepatitis C virus (HCV) infections are the most common causes of chronic liver disease in the world. Both viruses induce chronic hepatitis, which may progress to cirrhosis and eventually to hepatocellular carcinoma.1 It is estimated that there are 350 million HBV carriers and 170 million HCV carriers worldwide. HCV is an RNA virus of the Flaviviridae family and HBV is a DNA virus of the Hepadnaviridae family.2 HBV and HCV share modes of transmission, and their combined infection seems to be frequent, particularly in areas where the two viruses are endemic and among people at high risk for infection such as IV drug abusers, blood receivers like hemophiliacs and thalassemics, and by parenteral transmission.3,4 The diagnosis of HBV infection is usually based on the detection of hepatitis B surface antigen (HBsAg) in serum, and disappearance of this antigen indicates the clear ance of HBV. HCV infection is diagnosed by detection of anti-HCV and viral RNA in the serum.5 However, previous studies have shown that HBV DNA can be detected in patients with chronic liver disease who are negative for HBsAg but positive for antibodies to hepatitis B core antigen (anti-HBe).6-7 More recently, this so-called occult hepatitis B has frequently been identified in patients with chronic HCV infection. Patients with occult HBV and HCV co-infection usually have a delayed appearance, lower level, and shortened duration of HBsAg. Studies showed that HCV core protein is able to inhibit HBV replication, and for this suppressor effect the phosphorylated serines at position 99 and 116 seems to be essential. In addition, a high frequency of an eight-nucleotide deletion in HBV core promoter/distal X region was recently reported in patients with HCV and occult HBV infection, and this deletion mutation appears not to be present in patients with active HBV infection alone.8 Considerable data suggest that this occult infection is clinically relevant because it may be associated with severe forms of liver disease, poorly sensitive to interferon treatment and with a high risk of hepatocellular carcinoma development.9 However, whether the presence of such small amounts of HBS will lead to progressive disease has been questioned and indeed needs further confirmation from other areas of the world where HBV infection is rampant. Taking advantage of the fact that HBV and HCV infections are common in Iran, we determined the prevalence of occult HBV infection in patients with HCV-related chronic liver disease and studied the possible influence of occult HBV infection on the clinical outcomes of infected patients. PATIENTS AND METHODS Selection of cases
PCR-RT PCR
Serum and plasma samples from 207 referral patients to the molecular diagnostic lab of the Iranian Blood Transfusion Organization plus 130 cases as control were obtained by vacutainer system. All of the patients had a history of positive HCVPCR and HCV-Elisa. Both patient and case control samples were subject to HBV-DNA, HBsAg, HBcAb, HBcAg, HBeAb, HBsAb, ALT, and AST tests. None of them were under treatment. 173 of the patients were male and 34 female with age between 8-79 years old. Serological markers
Tests for HBsAg, anti-HBs, antiHBc and anti-HCV were done with commercially available kits (Avecina, Russia, Ortho, Dada Behring, Biorad, USA). Nucleic acid extraction
Plasma samples were frozen at -70°C before starting the nucleic acid extraction procedure. RNA was extracted preserved at -70°C. Serum was assayed for HCV-RNA by reverse-transcription-PCR with random hexamer and specific primer for 5´ untranslated region. The sensitivity of the assay was estimated by vqc panel ( less than 380 copy/mL). HBV-DNA was analyzed by 2 set primer for pre S conserved region. We used hot start method to decrease non-specificity and increase both sensitivity and specificity of the reaction. All precautions for avoiding PCR contamination were followed strongly. Each positive result was confirmed by a second independent PCR. PCR products for both HCV and HBV were electrophoresed on 1.8 % agarose. A 150 bp and 240 bp corresponded to positive PCR reaction for HCV and HBV genome. Serum ALT and AST level
HBV-DNA evaluation in HCV-RNA positive patients
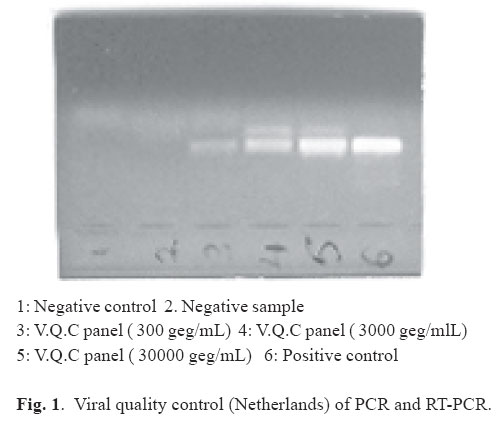
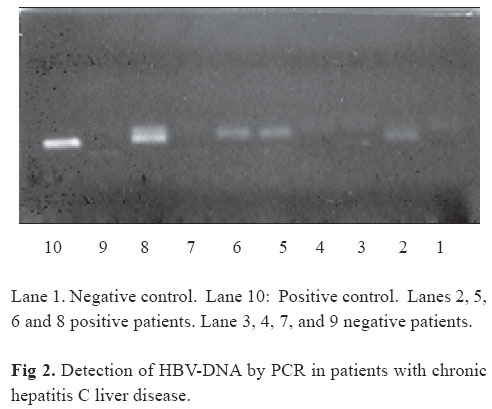
ALT and AST activity were estimated by Pars Azmun kit ( Tehran- Iran ) with a Hitachi auto-analyzer. RESULTS Of 207 patients with chronic hepatitis C (confirmed by Elisa-Riba and PCR) 23 patients (11.1%) were positive for HBV-DNA PCR for pre S region ( co-infection of HBV and HCV). Among co-infected patients 9.7 % were male and 1.4% female. Also the majority of patients were between 20-40 years old (47.8%). Table I characterizes the prevalence and distribution of co-infected patients. In addition 130 HBsAg, HBcAb, and HBsAb negative referral patients were also subject to HBV-DNA analysis. All cases were HBV-DNA negative according to vqc (viral quality control–Netherlands), and the sensitivity of our PCR and RT-PCR assay results was 300 and 380 geg/mL (Fig. 1). Occult versus co-infectedIn order to further clarify the nature of HBV-DNA positivity among the HCV-RNA population, we evaluated HBsAg status in this group. As Table I shows by modified Sacchi Chomzynski method (Trisol-LS, invitrogen-USA). Briefly 250 µL plasma plus 750 µL Trisol were mixed and 2 phase separate and RNA were precipitated with cold ethanol. Pellets were dissolved in 20 µL DEPC treated water. DNA was extracted by high pure viral nucleic acid kit (Roche, Germany) according to the manufacturer’s procedure. Both DNA and RNA were among this group 8.2% (17) of the 11% (23) who were HBV-DNA+ (HCV-RNA+) were HBsAg negative. For further characterization of HBsAg negatives we determined total anti-HBc for this group. Prevalence of anti-HBc positivity in Table II is shown. 53% (9/17) of HBsAg-, HBV-DNA+> , HCV-RNA+ patients have negative HBcAb and in contrast 47% (8/17) have positive HBcAb. According to our criteria the group with HBsAg (-), antiHBc(-) HBV-DNA (+), HCV-RNA (+) were suitable candidates for the occult HBV form (Fig. 2). According to Table II, males between 20-40 years old are the predominant group of occult HBV. As shown in Table III, no significant difference was found in epidemiological parameters in the two groups (HCV alone in comparison with HCV and occult hepatitis B co-infection). In the two groups, transfusion and IV drug use was the most frequent epidemiological characteristic. DISCUSSION
HBV infection is diagnosed when circulating HBsAg is detected.10 However, a unique persistent infection known as occult HBV infection, which is characterized by positivity for HBV-DNA in serum by using nested PCR assays, has been identified in HBsAg-negative pa-
HBV- DNA (+) A= % ———————————— Total no. of patients( 207 ) HBS-Ag (-) B= ———————————— Total no. of patients ( 207 ) Table II. Prevalence of Anti-HBc in occult hepatitis.
HBV- DNA (+) HBS-Ag (-) A= % ———————————— B= ———————————— Total no. of patients ( 207 ) Total no. of patients( 207 ) tients with or without serological markers of previous HBV infection ( anti-HBs or anti-HBc).11,12,13,14 Several recent studies have indicated that this occult HBV infection can be found in patients with chronic HCV infection at various frequencies.15,16,17,18 The high prevalence of occult HBV infection in such patients has been suggested to have clinical implications in the pathogenesis of HCV-induced chronic liver disease. The reason for disappearance of HBsAg is not well known, but in subjects co-infected with HCV, it seems that the HCV core protein can inhibit HBV replication15 HBV viral level in serum is usually less than 104 copies/mL in patients with occult infection which is significantly lower than in those with HBsAg positive infection.3 Thus we need a sensitive PCR technique for detection of this form of infection. Table III. Epidemiological characteristics of the two groups.
This study indicates a high rate of hepatic HBV-DNA turn-over in patient with HBsAg-negative chronic liver disease. Indeed when DNA-PCR results were analyzed, we found that 11.1 percent of patients with HBsAg-negative chronic liver disease had been detected by HBVDNA . Previous studies have shown that patients co-infected with occult hepatitis B and HCV suffer from a more severe disease. Studies have shown that patients with HCV and occult HBV had a significantly higher incidence of cirrhosis than those with HCV infection alone.16 Recent studies demonstrate that patients with occult hepatitis B and HCV infection have a poorer response to α-interferon compared to those with chronic hepatitis C alone.16 We investigated HBV infection in HBsAg negative patients with chronic hepatitis C. It seems the frequency of the occult form of HBV is significant in chronic hepatitis C. The prevalence of occult HBV infection was particularly high among patients with Anti-HBc antibodies. And we found that occult HBV infection co-infected with HCV was particularly high among patients at high risk for two viruses like multi-transfusion patients and IV drug abusers. REFERENCES
|
{kind=link}
{kind=link}