 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Medical Journal of the Islamic Republic of Iran , Vol. 19, No. 2, August, 2005, pp. 181-184 DETECTION OF HAEMOPHILUS INFLUENZAE TYPE B IN CEREBROSPINAL FLUID OF SUSPECTED CHILDREN WITH MENINGITIS BY PCR F.A. NAKHJAVANI,* Ph.D., F. BONAKDAR HASHEMI,* Ph.D., M.T.KALANI,* Ph.D., B. KAZEMI,** Ph.D., K. NOURI,*** Ph.D., N.AZADI,*** Ph.D., M. HAGHI ASHTIANI,**** Ph.D., M. ALIGHOLI,*M.S., U. ERFANI,**** M.S., AND M. ABEDINI,**** B.Sc. From the *Department of Microbiology, Faculty of Medicine, Tehran University of Medical Sciences, the **Department of Parasitology, Faculty of Medicine, Shahid Beheshti University of Medical Sciences, the ***Department of Biostatistics and Epidemiology, Faculty of Public Health & Institute of Health Research, Tehran University of Medical Sciences, and **** Children’s Medical Center, Microbiology Laboratory, Tehran University of Medical Sciences, Tehran, I.R. Iran. Corresponding author: M.Taheri Kalani, Department of Micro-biology, School of Medicine, Tehran University of Medical Sciences. Tel & Fax: 021-88955810, E-mail: taherikalani@razi.tums.ac.ir Code Number: mr05015 ABSTRACT Background: A polymerase chain reaction (PCR) assay with primers
from “hpd”gene was compared with culture for the detection of Haemophilus influenzae type
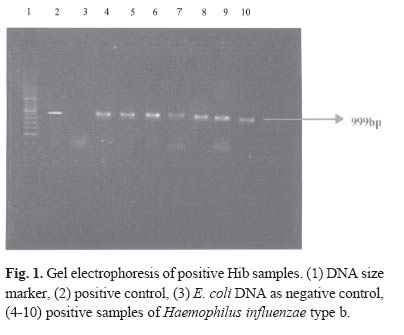
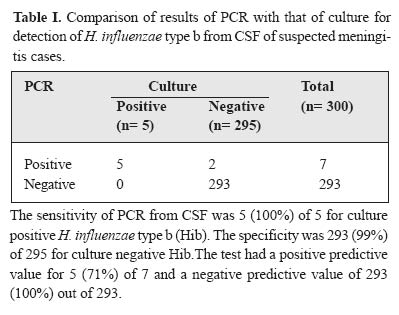
b (Hib) in CSF samples from children suspected of meningitis. Keywords: Haemophilus influenzae type b; Meningitis; PCR; culture; CSF; Iran; Incidence. INTRODUCTION Bacterial meningitis is a serious and sometimes fatal infection affecting the central nervous system.1 Haemophilus influenzae type b (Hib) is an important cause of meningitis, resulting in significant morbidity and mortality in children aged less than five years in Bacterial meningitis is a serious and sometimes fatal countries where children are not vaccinated against Hib.2 infection affecting the central nervous system.1 Encapsulated strains are responsible for a variety of Haemophilus influenzae type b (Hib) is an important invasive diseases, the most frequent being meningitis, but epiglottitis, arthritis, pneumonia, and cellulitis also occur.3 A recent study in Children’s Medical Center in Tehran during 2001-2002 showed that Hib is the cause of 15.6 % of cases of bacterial meningitis. The exact burden of invasive Hib disease in Tehran is unknown, since optimum and rapid laboratory facilities are not routinely available for detecting the etiologic agent of meningitis, the most important disease caused by Hib.2 In many industrialized countries, the incidence of invasive Hib disease has fallen sharply with the introduction of Hib conjugate vaccines into routine immunization programs.2 Since the widespread use of Haemophilus influenzae capsular type b (Hib) conjugated vaccines in the United States began in 1987, the incidence of invasive Hib disease in children less than 5 years old has declined drastically.4 Despite the success of the Hib vaccination program, the re-emergence of invasive Hib disease has been noted in a well vaccinated population, implying the necessity for continuous surveillance in the post-vaccination period.3 Diagnosis of acute bacterial meningitis by direct microscopy is rapid but non-specific and has a low sensitivity. On many occasions, it fails to provide definitive evidence of infection due to a particular species.2 Traditional laboratory diagnostic methods (Culture-CSF) take up to 36 hours or more and may show negative results in approximately 30% of cases due to antibiotic use prior to sampling.4 Furthermore, it has been observed that following an increase in the practice of starting antimicrobial therapy prior to clinical samples collection, the ability to confirm the pathogenic microorganisms of bacterial meningitis has decreased by approximately 30%. The need for rapid, sensitive and specific methods for the diagnosis of meningitis due to Hib is becoming more urgent, since strains of Hib resistant to ampicillin, chloramphencol, and co-trimoxazole, emerged in different parts of the world, questioning the appropriateness of empirical antimicrobial therapy. Moreover, estimation of the burden of Hib disease and the efficacy of Hib vaccination is imprecise without an opti-mum diagnostic test.5 The development of a PCR assay for target gene amplification has enabled the detection of low numbers of pathogens in clinical samples.5 We carried out this study to detect Hib directly from the CSF of patients suspected of meningitis by culture and PCR assay. MATERIAL AND METHODS Study populationThe study population included children less than five years old admitted to Children’s Medical Center of Tehran. CSF samples of 100 μ L were gathered from suspected cases. A child with signs and symptoms of meningitis, such as high fever, lethargy, convulsions, bulged fontanelles, neck stiffness, etc., was considered a case of meningitis, and a lumbar puncture (LP) on that child was obtained.5 Clinical samples300 Cerebrospinal fluid (CSF) samples were collected for detection of Hib with PCR and culture (Leventhal and Chocolate Agar medium). Laboratory diagnosis of HibPatients with suspected bacterial meningitis were subjected to lumbar puncture for collecting CSF. All CSF samples were cultured on Chocolate Agar and Leventhal medium. The suspected bacterial colonies were identified by typical Gram stain morphology, catalase, oxidase and requirement test of factors X and V.4 The Haemophilus influenzae isolates were serotyped by Hibspecific antiserum.8 Detection of Hib by PCROne hundred μ L of CSF was taken in a microcentrifuge tube and was heated in a boiling water batch for 15 minutes and centrifuged at 10000 g for 1 minute. Ten μ L of supernatant was used as template DNA.8 PCR primers The selection of primers was based on the published work of Sasaki and Munson. The primers were constructed from the “hpD”gene encoding outer membrane protein, which acts as a glycerophosphodiester phosphodiesterase. The primers for detecting Hib were Haem Right (primer 1) [5`CAGTAAATACACCTGTTGCCCCTG-3`], and Haem Left (primer 2) [5`-GCCATTCATCAAATA-3`], and were similar and complementary to the nucleic acid sequence of conserved regions of the “hpD”gene specific for b serotype of H. influenzae. Both primers were comprised of 24 bases.8 PCR assayPCR was performed in a reaction mixture of 50 μ L containing 1.5 μ L ( 1.5 mM) MgCl2, 1 μ L (0.2 mM) dNTP, 5 μ L (1X) 10X PCR buffer (KCl,Tris-HCl, Magnesium), 0.5 μ L (2.5U) of Taq DNA Polymerase (Cinnagen, Lot.810017), 10 μ L DNA Template (Haemophilus influenzae, ATTC 35056 Difco as control positive), 40 μ L D.W, and primers (Primers 1,2: 2 μ L or 40 pm) per reaction tube. The reaction mixture was processed in a programmable DNA thermal cycler (Ependorff, Germany) consisting of 35 cycles with the following parameters: (a) denaturing for two minutes at 94oC, (b) annealing for two minutes at 56oC, and (c) extension of primers for two minutes at 72oC. The primary denaturaton took 10 minutes at 94oC and final extension 8 minutes at 72oC. At the end of 35 cycles, the samples were kept at 4oC until analyzed. PCR products for Hib were detected by 1.5 % agarose gel electrophoresis. RESULTSOver a period of one year (Dec. 2001- Dec. 2002), 300 children suspected of meningitis aged less than five years were included in the study. Hib was isolated from CSF cultures. Five of the 300 CSF samples were positive for Hib, both by culture and CSF-PCR. The latter also detected Hib in 2 of 295 culture-negative CSF samples (Fig 1). Compared to the CSF culture results, CSF-PCR yielded 2 false positive and no false negative results (Table I). The sensitivity and specificity of CSF-PCR was 100% and 99%, respectively. Based on PCR and culture results the incidence of Hib among children referring to the Children’s Medical Center of Tehran were 2.4% and 1.7% respectively. Based on culture results, 15.6% of the cases of bacterial meningitis in children were due to Haemophilus influenzae type b. Age at diagnosis ranged from 10-42 months (median, 22 months). Incidence among males and females based on culture and PCR results were 20%, 14% and 80%, 86% respectively. DISCUSSIONPCR is increasingly being used in clinical microbiology laboratories for the detection of agents of infectious disease, since the conventional diagnostic methods, such as microscopy, culture, and serology, fail to identify the responsible pathogen in many occasions.10 In the present study, we found PCR to be a useful technique for the detection of Hib “hpD”DNA in the CSF samples from suspected meningitis patients. The “hpD”gene has been used as target DNA for amplification by PCR. The primers were sensitive and specific for the detection of Hib in CSF samples. The selected primer showed excellent specificity with non-Hib strains. PCR was also negative with other common agents of meningitis such as Pneumococcus and S. agalactiae. It provided a result within a day from the clinical samples, whereas the culture methods took up to 36 hours or more. In a recent study, the DNA extraction method of Shoma et al. was used for CSF samples.12 The limitation of the study is that we used agarose gel electrophoresis for screening PCR products, which appears to be a less-sensitive method for detecting PCR products than hybridization.1,4,12 DNA extraction by a commercial kit may also increase the yield of DNA sufficiently for PCR amplification. It has been observed in our clinical microbiology laboratory, as in many other laboratories,12 that there is a growing discrepancy between the numbers of clinically suspected and culture-confirmed cases of bacterial meningitis. To address this problem, non-culture methods, such as CSF-PCR, have been employed and shown to detect additional cases of Hib meningitis in our study. CSF-PCR showed a sensitivity of 100% compared to the conventional culture method. Thus, the sensitivity of CSF-PCR was superior to that of bacterial culture. It is a good diagnostic test for the detection of Hib in CSF samples. It is relatively simple and requires a short period of time compared to culture. However, determining the antibiotic susceptibility of Hib isolates is a problem in the PCR technique. Further development of a multiplex PCR for detecting both Hib and the antibiotic resistance gene would be extremely useful.12 Both culture and PCR tests detected Hib in CSF samples. We did not detect other serotypes of H. influenzae by culture from CSF, suggesting that Hib is the primary cause of invasive infection such as meningitis among children in Tehran. Following diagnosis of meningitis, administration of early therapy with a proper antimicrobial agent is the key factor to reduce mortality and morbidity and sequels of invasive Hib disease, particularly meningitis. ACKNOWLEDGEMENTSWe would like to thank the staff of the microbiology laboratory of Children’s Medical Center of Tehran, for their help and advice and the Department of Microbiology, Faculty of Medicine, Tehran University of Medical Sciences for financial support of this investigation. REFERENCES
Copyright 2005 -Medical Journal of the Islamic Republic of Iran |
{kind=link}
{kind=link}