 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
VULVAR CARCINOMA IN PREGNANCY:A CASE REPORT MITRA MODARES GILANI, M.D.,* MALIHE HASANZADEH, M.D.,** AND NADEREH BEHTASH,* M.D. From the Gynecology/Oncology Department, Tehran University of Medical Sciences, Tehran, I.R. Iran. *Associate Professor, of Gynecology Oncology, Tehran University of Medical Sciences,
Tehran, Iran. Code Number: mr05016 ABSTRACTCarcinoma of the vulva has commonly been recognized as a disease of postmenopausal
women, but some cases have been reported in young women during pregnancy.
A 28-year-old Afghan woman in her sixth pregnancy presented with a vulvar lesion. Subsequent biopsy revealed squamous cell carcinoma. The patient was treated with local excision. She had a cesarean section in her 36th week of pregnancy. She underwent modified radical vulvectomy with bilateral groin dissection four weeks after cesarean. Because of a grossly positive groin lymph node, she also underwent radiation therapy. She is alive without invasive cancer 7 months after diagnosis. This case demonstrates the need to biopsy all suspicious vulvar lesions, even in young and pregnant women. Keywords: Vulvar carcinoma, pregnancy, squamous cell carcinoma of vulva. INTRODUCTION Vulvar cancer is an uncommon cancer representing approximately 4% of female genital tract cancers.1 Vulvar squamous cell carcinoma( SCC) is predominantly a disease of postmenopausal women & is rarely observed during pregnancy.2 Fewer than 20 cases of vulvar carcinoma diagnosed and treated during pregnancy, have been reported.3 Vulvar carcinoma in younger patients is related to human papillomavirus ( HPV) infection and smoking and is commonly associated with VIN.4 The association between immune suppression and vulvar cancer in younger women has been reported.5 Because no series of a meaningful size have been reported, management is individualized. 2 Surgical management during pregnancy depends on several factors: gestational age at diagnosis, lesion size, its depth and location & lymph node status.6 Most cases were treated with radical vulvectomy, bimlateral inguinal lymphadenectomy and standard surgical therapy during their pregnancies. The pregnancies weren’t terminated. With lymph node metastasis, radiation therapy was given after delivery by cesarean section. 7 CASE REPORT
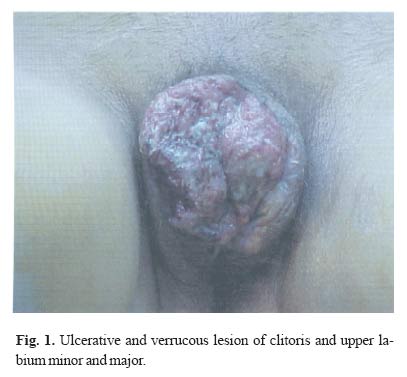
In January 2004, a 28-year-old Afghan woman (gravid 6, para 5) referred to Vali-e-Asr hospital complaining of a 10 week history of progressive itching and swelling on her vulva. She had a history of recurrent vulvar lesions in three previous pregnancies, from 10 years ago. She had a histology of condyloma and HPV infection in her 5th pregnancy 3 years ago. In this patient HPV infection was one of the risk factors for vulvar carcinoma. In spite of an abnormal vulvar lesion, she was treated by topical antibiotics and had not undergone biopsy. Physical examination revealed a 7*8 cm raised verrucous and necrotic lesion overlying the clitoris and upper labia major (Fig. 1).She had palpable bilateral inguinal lymph nodes. Gestational age was not clear because she had no antecedent prenatal care. Ultrasound examination revealed a singleton fetus of 32 weeks gestational age. Cervical cytology was negative. Full sexually transmitted infection screen was performed and was negative including HIV, syphilis serology & Hemophilus ducreyi culture. Histology was well differentiated SCC. The patient underwent excisional biopsy after one week. Histological exam of the specimen was SCC. Surgical margins of the lesion (2cm) were free except for the left lateral margin. Therapy was complicated by superficial wound breakdown, 4 weeks later. At approximately 36 weeks of gestational age, the patient delivered a 2800 gram infant by cesarean section with Apgar scores of 7 and 9 at one and five minutes, respectively. The patient didn’t have any positive pelvic node and pelvic lymphadenectomy wasn’t performed. On her 21st postpartum day, the patient underwent radical vulvectomy with bilateral inguinal and femoral lymphadenectomy. Lymph nodes were positive for metastatic disease. She received radiotherapy and 3 courses of chemotherapy (Vincristin 1 mg/m2 and Cisplatin 50 mg/m2). Seven months after treatment, the patient remains without evidence of recurrent disease. DISCUSSION
Invasive squamous cell carcinoma of the vulva is rarely seen during pregnancy.1,2 While a causative agent for lower genital tract cancer has never been identified, risk factors for the development of vulvar neoplasia resemble those associated with squamous cervical cancers. Additionally, syphilis, herpes genitalia and chronic granulomatous disease (lymphogranuloma venereum) are of possible etiologic significance.4 Recently much attention has been focused on the close association between human papilloma virus (HPV) and vulvar carcinoma. Carter reported 27 cases of vulvar carcinoma and found that 20 patients (80%) were smokers. Associated medical and immunosuppressive conditions present in these patients included vulvar HPV (n= 3), diabetes mellitus (n= 3), pregnancy (n=2), autoimmune connective tissue disease (n= 2), renal transplant (n= 2), previous chemotherapy for invasive malignancies at other sites (n= 1), chronic hepatitis (n= 1), schizophrenia (n= 1), and one patient on Imuran for herpes zoster and multiple sclerosis. The conclusion was that while invasive vulvar tumors are uncommon in young women, smoking and a history of an immunosuppressive medical illness is common in this patient population.5 A pregnant woman with a vulvar malignancy presents a significant challenge for the clinician for many reasons. Considerable diagnostic delay is common due to confusion of symptomatology with the physiologic changes associated with the pregnant state. In addition, difficult medical, ethical, and religious issues arise when the treatment of these malignancies is incompatible with continuation of the pregnancy. Unfortunately, a relatively limited experience with cancers in pregnancy has prevented the development of universally accepted management algorithms for diagnosis and many of the complex issues regarding their treatment.8 A rational management plan applicable to most patients is unavailable and treatment of vulvar cancer coexistent with pregnancy must be highly individualized, with attention to several parameters such as stage, lesion size and location and gestational age.6 Vulvar carcinoma in pregnancy is usually stage I or II disease. Radical surgical treatment is the mainstay of therapy during the first two trimesters.9 Surgical morbidity is proportional to genital vascularity, which increases through pregnancy. Barclay reported no immediate adverse results in any patient receiving antenatal treatment, although one patient eventually required cesarean section delivery for vulvar scarring.10 Selecting an appropriate mode of delivery must also be individualized. Most authors recommend treatment at any time up to 36 weeks of gestation. In some cases, delaying treatment to the postnatal period, resulted in a stormy course and eventually the patient’s death due to disease recurrence.4 Our patient was a young woman, with vulvar carcinoma which had occurred in pregnancy. She underwent local excision and optimal treatment was delayed until the postpartum period. Perhaps, local excision and chemotherapy in the late trimester is a good option in vulvar carcinoma during pregnancy. In addition, this case also emphasizes the need to consider malignancy as a differential diagnosis in vulvar lesions of young women. We should biopsy all suspicious vulvar lesions, even in young and pregnant women. Early and thorough diagnosis with subsequent appropriate definitive treatment cannot be overemphasized. REFERENCES
Copyright 2005 -Medical Journal of the Islamic Republic of Iran |
{kind=link}