 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Medical Journal of the Islamic Republic of Iran , Vol. 20, No. 1, May, 2006, pp. 1-3 Original Articles CONGENITAL MUSCULAR TORTICOLLIS: EVALUATION OF SURGICAL TREATMENT IN FIFTEEN CONSECUTIVE PATIENTS S.M. MAZLOUMI, M.D., N. MOKHTARI AMIRMAJDI, M.D., * AND G.R. BAHADORKHAN, M.D. From the Depts. of Otorhinolaryngology, Orthopedic Surgery and Neurosurgery,
Mashhad University of Medical Sciences, Mashhad, I.R. Iran. Code Number: mr06001 ABSTRACT Background: The main objective of this study was to define
the clinical changes of facial deformity in patients older than 5 years with
congenital torti-collis treated by proximal and distal sternocleidomastoid
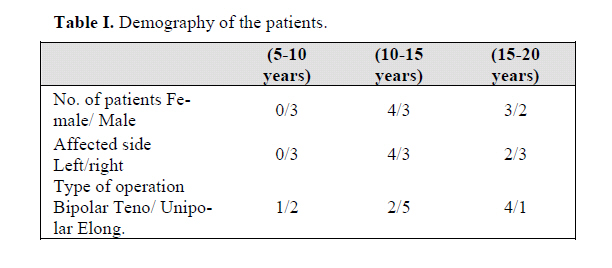
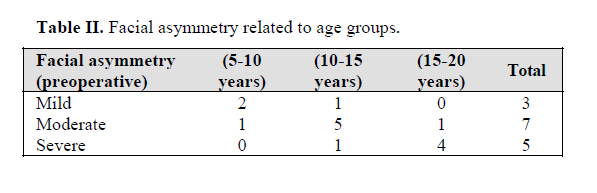
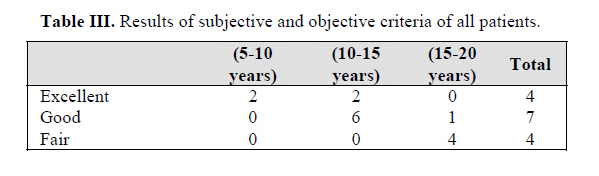
tenotomy. INTRODUCTION A soft tissue swelling over the sternocleidomastoid muscle is noticed during the first week of life in approxi-mately 20 percent of all patients who have congenital muscular torticollis (CMT).1 Cosmetic deformity and limitation in neck movement causes most patients to seek medical care, but late seque-lae such as facial asymmetry, cervical scoliosis, and dis-turbed vision can occur. A preponderance of involvement of the right side compared with the left side of approxi-mately 15 percent has been reported in patients who have congenital muscular torticollis.2, 3 Macdonald further divided CMT into sternomastoid tumor group (SMT) and those with tightness of the sterno-cleidomastoid muscle but no clinical tumor appearance as muscle torticollis (MT).4 Postural torticollis (POST) was used to describe those with congenital torticollis with all the clinical features of torticollis but with no demonstrable tightness nor tumor of the sternomastoid muscle.5 Congenital muscular torticollis has to be differentiated from torticollis due to congenital anomaly of the atlas6, atlanto-axial subluxation due to inflammation around the neck, disease of the eye (superior oblique muscle palsy)3, 7 and from spasmodic torticollis. The reported incidence of torticollis varies from 0.3% to 1.9%.8 Treatment includes observation, application of an orthosis, gentle manual stretching, and various types of surgical procedures. Some investigators showed that risk factors of surgery was responsible for delayed attempt at surgery in the SMT group and the clinical type with severe head tilt.9 The purpose of this study was to evaluate the effec-tiveness of biterminal open release and muscle elongation of the sternocleidomastoid muscle on resolution of facial asymmetry, in patients who were over 5 years of age. MATERIAL AND METHODS The current study is a retrospective study of all CMT patients operated on in one center over eighteen year pe-riod. Patients with congenital anomalies of the cervical spine, spasmodic torticollis, and other forms of neuro-genic, ocular and organic torticollis were excluded from the study. All patients had muscular torticollis without palpable or visible tumor but with clinical thickening or tightness of the sternomastoid muscle on the affected side. Preoperative radiographs of the cervical spine, which had been made for all of the patients, were available for twelve patients at the time of the last follow-up. Cervico-thoracic scoliosis was present in all patients. Radiographs of the cervical spine in two planes were included in the follow-up examination. Hip dysplasia and congenital anomalies of foot was not present in our patients. In seven patients a uniform method of proximal (cephalad) and distal (caudad) open release and partial excision of the clavicular and sternal heads of the sterno-mastoid muscle were performed and in eight patients elongation of the sternal and clavicular head of the muscle were performed. Postoperatively, 5-7 days of cervical traction followed by an intensive program of physiother-apy was prescribed that included scar treatment, mainte-nance of full passive range of motion of the neck, and active strengthening exercises for a period of 3 to 4 months. There were no complications intraoperatively or postoperatively in our patients. At the final assessment the overall results were graded by a scoring system based on both subjective and objective criteria and grouped as ex-cellent, good, and fair, respectively. The subjective score was based on interviewing the patients at the final follow-up and inquiring about the overall cosmetic and functional results of the patients. RESULTS Nine patients were male and six female. Facial asym-metry was equally distributed in all of the age-groups. The right sternocleidomastoid muscle was affected in ten pa-tients and the left in five patients. All patients had muscu-lar torticollis without a visible tumor in the sternocleido-mastoid muscle (MT group). The age of the patients at the time of operation ranged from 5 years to 20 years (average approximately 8.8 years). Most patients were operated on between the age of 10 and 15 years. Four patients (28.5%) were adults at the time of operation. Seven of fifteen pa-tients in whom congenital muscular torticollis had been treated with biterminal tenotomy were followed between 2 and 6 years and eight patients in whom elongation of the sternocleidomastoid muscle was done were followed for 3 to 7 years postoperatively. Demography of the patients is shown in Table I. Preoperatively, facial asymmetry had been graded as mild in three patients, moderate in seven patients and se-vere in five patients (Table II). All of the patients had full flexion and extension of the cervical spine at follow-up examination. Lateral bending toward the untreated side was limited in twelve patients (80%). The limitation was 10 degrees or less in four of these patients and 20 degrees in eight patients. These pa-tients were over ten years old and mostly over fifteen years. Four patients had limitation of rotation of the head toward the treated side; it was limited to 10 degrees in three and 20 degrees in one patient. The patients felt more handicapped by limitation of rotation than by limitation of bending. Asymmetry had thus improved by one or two grades in more than ten of the patients. The asymmetry improved more often in younger patients. The longer the postopera-tive interval, the more the asymmetry was noted to have improved. This relationship between improvement and the postoperative interval was most obvious in patients oper-ated on at the age of five to ten years (five patients). Compared with the findings on preoperative radio-graphs that were available for twelve patients, these find-ings suggested complete resolution of the scoliosis in one half of the patients. However, scoliosis improved more rapidly in younger children than in older patients. The results of subjective and objective criteria at fol-low up are shown in Table III. DISCUSSION If congenital muscular torticollis persists beyond the age of one year, it does not resolve spontaneously. Chil-dren with torticollis who were treated during the first year of life had better results than those treated later, and an exercise program was more likely to be successful when the restriction of motion was less than 30 degrees and there was no facial asymmetry. Non-operative therapy after the age of one year was rarely successful.10 Controlled manual stretching is safe and effective in the treatment of CMT when a patient is seen before the age of one year. In this age group only 8-10% of patients required surgery.11 Shim et al. treated CMT surgically in 32 patients over 8 years of age who had not received any prior medical treatment. They concluded that in patients older than school age, even for those who have finished growth, suf-ficient unipolar or bipolar release of the sternocleidomas-toid muscle and intensive postoperative care are expected to yield satisfactory treatment results.12 An assessment with three-dimensional computed to-mography imaging for craniofacial deformity in patients with uncorrected CMT showed that the cranium and cra-nial base deformity occurred early in patients with uncor-rected torticollis, while the facial bone deformity occurred in the childhood stage. The cranial and facial deformity became more severe with age. Early release of the muscle restriction is advised to prevent craniofacial deformation.13 Results of this study showed that elongation of the sternocleidomastoid muscle at the distal pole was effective in young patients below 10 years old. In patients older than ten years tenotomy and release of the proximal and distal head of the sternocleidomastoid muscle was effec-tive in movement of the neck but was not effective for reduction of the facial asymmetry. REFERENCES
Copyright 2006 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr06001t2.jpg] [mr06001t3.jpg] [mr06001t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}