 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
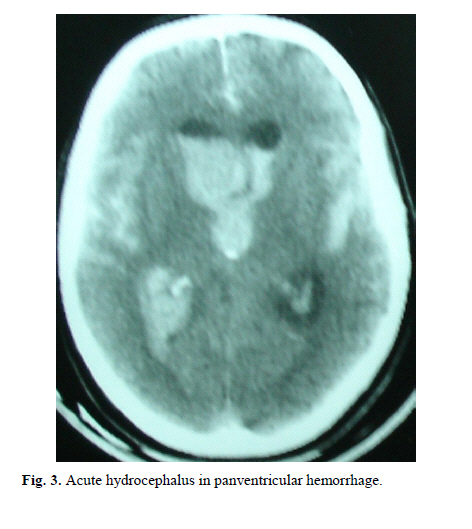
Medical Journal of the Islamic Republic of Iran , Vol. 20, No. 1, May, 2006, pp. 13-18 TRAUMATIC INTRAVENTRICULAR HEMORRHAGE IN SEVERE BLUNT HEAD TRAUMA: A ONE YEAR ANALYSIS G.R. BAHADORKHAN, M.D. * From Dept. of Neurosurgery, Mashhad University of Medical Sciences, P.O. Box 91375-3983, Mashhad, I.R. Iran. Code Nuber: mr06004 ABSTRACT Background: High resolution CT scan has made early diagnosis of intra-ventricular hemorrhage (IVH) easier. Posttraumatic intraventricular hemor-rhage has been reported to a greater extent because of the CT scan. Keywords: Intraventricular hemorrhage, Traumatic intraventricular hemorrhage, Severe head injury, Ventricular hemorrhage. INTRODUCTION High resolution CT scan has made early diagnosis of intraventricular hemorrhage (Figs 1, 2, 3, 4) easier and post-traumatic intraventricular hemorrhage (IVH) has been increasingly reported.1 The actual origin of IVH has rarely been identified and the pathogenesis and mechanisms in-volved are still obscure. Although different speculations have been proposed,2 the incidence of IVH in nonpenetrat-ing head injury is 1.5 to 3% and 10 to 25% of patients with severe head injury (GCS less than 8) have IVH.3-6 The presence of IVH indicates that a severe force has been applied to the head and generally is a sign of severe head injury.2, 3 Poor prognosis in this condition is a reflection of the severity of the injury to the head. Intracerebral hemor-rhage (ICH) and basal ganglia hemorrhage usually find a way to the ventricles.5, 7, 8 In the absence of intra-parenchymal hemorrhage IVH is most often caused by tearing of the subependymal veins in the fornix, septum pellucidum or choroid plexus found in autopsy studies.1, 2 Posttraumatic IVH rarely produces hydrocephalus,1-4, 8 and the presence of IVH in a patient with image-proven dif-fuse axonal injury (DAI) shows that other pathological mechanisms are involved.9, 10 Prognosis is poor in these patients and it is not known whether it is due to the pres-ence of blood in the ventricle per se, due to induced hy-drocephalus or increased intracranial pressure.3, 10 This-prospective study in severe head injury victims with IVH hopes to determine the incidence and prognosis and it's correlations with accompanying brain injuries and dis-cusses the probable mechanisms involved. PATIENTS AND METHODS In this one year prospective study (March 2001-2002) 1117 cases of severe head injuries (with a GCS less than 8) were admitted to the Neurosurgical Intensive Care Unit (NSICU) of Kamyab Hospital, the main trauma center in Mashhad, Iran. Kamyab Hospital is affiliated with Mash-had University of Medical Sciences offering trauma emer-gency medical care to almost 5 million residents and 12 million visitors each year. 203 of these patients had extra-cranial lesions (i.e. facial, spinal, limbs, abdomen, thoracic or injuries to other parts of the body and were omitted from this study.) The remaining 31 cases of a total of 904 patients (3.4%) had IVH with or without concomitant CT abnormalities and without extra-cranial lesions. The pri-mary CT scan in the remaining 31 cases was done within the first six hours of admission and repeated if the patient survived during the first 24 hours and then as needed dur-ing the next days or weeks. Of the surviving patients a controlled enhanced CT scan or MRI was performed to access the other possibilities or causes of hemorrhage such as arterio-venous malformations (AVM) and aneurysms. There was no history of hemorrhagic tendency and no intravenous site of abnormal bleeding noticed in any of these patients. Bleeding time, clotting time, prothrombin time, PTT and platelets were normal and if abnormal were excluded from this study. All the patients were admitted to the NSICU and if needed, ventilator support was done with a volume limited ventilator and an average of arterial pCO2 of 30-35 mmHg was maintained. Mannitol (1 gr/kg as bolus over 30 minutes and 0.25-0.5 gr/kg q6h) and fu-rosemide (10-20 mg IV q6h) was started judiciously. None of the patients had intracranial pressure monitoring or had undergone barbiturate therapy or received steroids. For each case, age, sex, skull x-ray and CT abnormalities, mechanism of trauma, probable site of trauma and mecha-nism of impact, Glasgow Coma Scale (GCS) on admis-sion, treatment modalities and final outcome according to Glasgow Outcome Scale (GOS) were recorded and analyzed. RESULTS Two groups of patients with traumatic IVH were iden-tified, those with probable known site of origin of IVH and those in whom it was not known. Of the 31 cases with traumatic IVH, in 18 cases detection of the original hem-orrhage was possible; in the remaining 13 cases the site of the hemorrhage could not be determined. In the first group a hemorrhage focus was found near or adjacent to the ven-tricles and had found its way to the ventricles. In the con-tusion group (CG) 9 cases had intra-cerebral hemorrhage, 4 cases in the frontal lobe, 3 cases in the temporal lobe and 2 cases in the parietal lobe that had found a way to corresponding horns of lateral ventricles (Fig 4). In the contusional group, motor vehicle accidents (6 cases) were the most common cause, 2 cases from assault and 1 case was from a fall (Table 1). 5 cases had hemorrhage in the caudate nucleus and 4 cases had hemorrhage in the thala-mus (Fig.2), called the basal ganglia hemorrhage group (BGHG) (3 car collisions, 3 hit by cars, 1 hit by a motor-cycle, 1 assault and 1 fall). Of the remaining 13 patients in whom the origin of traumatic IVH was not determined 7 cases had hemorrhage around the brain stem, peri-brain stem hemorrhagic group (PBSHG), and 6 cases had minor intracranial lesions (MICLG), like multiple small in-tracerebral or corpus callosum hemorrhages, insignificant SDH, EDH or subdural effusions. Those with a hemor-rhage around the brain stem had different brain stem signs such as irregular pupils, fixed or dilated pupils and respi-ratory irregularities. 3 cases had pan-ventricular hemor-rhage and 20 cases had hemorrhage in lateral ventricles, while in 2 cases IVH was confined to the lateral and 3rd ventricles; in 6 cases hemorrhage was slight (less than 5 mL) and limited to the lateral ventricles. Major hemorrhage in addition to IVH was found in 14 cases, 4 cases had epidural hematoma (EDH), 4 cases had subdural hemorrhage (SDH), and 7 cases had a combina-tion of ASDH. EDH and contusional prarenchymal hem-orrhage all needed surgical evacuation. 7 cases had differ-ent insignificant intracranial abnormalities (i.e. minor epi-dural hematoma, minor sub-dural hematoma, sub-arachnoid hemorrhage, minor cortical contusion and sub-dural effusion) which did not need surgical intervention. 18 surgical procedures for accompanying intracranial hemorrhage were done in 14 cases. (6 epidural hematoma, 4 sub-dural hematoma, and 7 a combination of intra-parenchymal hemorrhage with ASDH and/or EDH and 4 cases underwent two surgical procedures, one for bilateral EDH, one for contralateral SDH to the original EDH, one for ICH ipsilateral to EDH and one for SDH contralateral to right original SDH). External ventricular drainage for acute hydrocephalus was done for cases 4 and 7 (Figs 1 and 3). From nine cases with ICH and different accompanying intracranial lesions (CG) which underwent surgical proce-dures, 5 cases expired (55.5%), 2 cases developed severe disability (22.2%) and 2 cases have mild disability (22.2%). Of the 7 cases with caudate nucleus hemorrhage 3 died (50%), 2 developed moderate disability (33.3%) and one is in a vegetative state (16.7%). In three cases with thalamic hemorrhage one died (33.3%), one had se-vere disability (33.3%) and one had moderate disability (33.3%). Of the 7 cases with hemorrhage around the brain stem (PBSHG) 5 cases died (71.5%), one had severe dis-ability (14.2%) and one is in a vegetative state (14.2%). All 7 cases within this group (PBSHG) had acceleration deceleration in anterior-posterior direction due to motor vehicle accident (3 in car collision, 2 were hit by a car, and 2 in motorcycle accidents). Of 6 cases with slight IVH and minor intracranial lesions (MICLG) one died (16.7%), three. developed mild disability (50%) and two have recov-ered well. Both of acute hydrocephalic cases who needed external ventricular drainage expired (Figs 1and 3) (Table 1). Age range of patients was from 3 to 84 and the major-ity of patients were in the 2nd and 3rd decade of life with a mean age of 30 years. There were 24 male and 7 female patients. The most common causes in these cases were motor vehicle accidents (26 cases, 84%), and the least common cause was from assault (3 cases, 10%) and from a fall 2 cases (6%) (Table 1). DISCUSSION Intraventricular hemorrhage causes brain damage by cerebral spinal fluid circulation (CSF) impairment, caus-ing ventricular size enlargement (hydrocephalus) and in-creased intracranial pressure and may cause additional damage to the surrounding brain tissues. In evaluating intraventricular hemorrhage other causes such as hyper-tensive intracerebral hemorrhage extending to the ventri-cles, rupture of the intracranial aneurysms, and vascular malformation, systemic bleeding tendencies and neonatal germinal matrix hemorrhage should be considered and differentiated from pure traumatic IVH. Due to deficient fibrinolysis and hemolysis of CSF the spontaneous re-moval of IVH is very slow. Current treatment modalities include external ventricular drainage and more recently the controversial administration of fibrinolytics such as tissue plasminogen activators. Although both treatments can expedite the clearance of IVH but no conclusion can be drawn from the effect on clinical outcome.11 Introduc-tion of computerized axial tomography and especially the high resolution tomography and its widespread use in acute head injury has made IVH more easily diagnosed and consequently much more reported. Also revealing IVH to be more common than was previously thought.12.13 High resolution CT scan has made it possible to recognize the probable site of head injury and if these findings are compared with autopsy findings the pathogenic mecha-nism of traumatic IVH especially in patients who survived can be determined.1-3, 14 Cordobes et al. mentioned the most common mechanism of IVH in head injury was the spread of blood in to the ventricle from nearby contusion hemorrhage.4 In this study 31 cases of traumatic IVH in severe closed head injury were studied and analyzed for age, sex, cause of trauma, GCS on admission, CT find-ings, treatment modalities, probable site of impact and final outcome for each case. A poor outcome is obtained from this study because only patients with severe head injury (GCS less than 8) were included (15 died, 8 mild disability, 4 severe disability, 2 vegetative state, and 2 good recovery). If we had included all grades of patients with head injuries from mild to moderate to severe blunt head injuries with IVH a more favorable outcome would have resulted (subject of another study). Nine cases in this study had contusional intraparenchymal hemorrhage as the cause of IVH and in the remaining 22 cases other mechanisms were involved. In the contusional group, in contrast with the basal ganglia hemorrhage group, the impact and the intracranial lesion were on the lateral side while in the basal ganglia group the lesion which almost corresponded to the impact side are more posterior (oc-cipital) for thalamic and anterior (frontally) for caudate nucleus hemorrhage. In this basal ganglia group there was concomitant lateral or polar impact. Zuccarello et al12 de-scribes the central cavitations as a cause of IVH which occurs with a delay mode. This could not occur in our study since all of the study cases had IVH in the first six hours. Tearing of the sub-ependymal veins usually cause hemorrhage in the sub-ependymal areas1-3 and this had not occurred for the basal ganglia group where the hemor-rhage was confined to the caudate nucleus or thalamus. Early appearance of basal ganglia hemorrhage and poste-rior-anterior direction of trauma suggest a shearing injury between the nuclei and perforating vessels plays a role in the pathogenesis of caudate and thalamus hemorrhage and spread to ventricles.3, 4, 15 Perforating vessels originating from major cerebral arteries have their major curve in the coronal plan and supply the basal ganglia and vulnerable to impact along the long axis of the skull. Although the putamen and insula are supplied by the perforating vessels from the proximal part of the middle cerebral artery but traumatic IVH is rare in these regions and seldom cause IVH.16, 17 Injury in the brain stem is almost always seen with hemorrhage around the brain stem2, and causes a poor outcome. This group (PBSHG) of patients in the pre-sent study had irregular or dilated fixed pupils with differ-ent respiratory abnormalities from the very beginning of the trauma and three of them had concomitant intracranial traumatic lesions which needed surgical removal. All 6 cases within this group had acceleration deceleration in an anterior-posterior direction due to motor vehicle accident in which tearing of sub-ependymal veins is thought to occur through the generation of a negative pressure when an impact along the sagittal diameter of the skull deforms the skull by increasing the minor axis, increasing ventricu-lar diameter1-3, 18, 19 (3 in car collision, 2 hit by cars, and 2 in motor cycle accidents). In this group a direct cause of IVH was not detected although tearing of large sub-ependymal veins can not be ignored.3 What is described by Tsai et al.20 as an irregular sub-ependymal enhance-ment before rupture of ependyma to produce IVH was not detected in any of the 31 cases. In those 6 cases (case numbers 26 to 31) who had slight IVH less than 5 mL and/or confined to a part of the ventricle with or without minor cranial lesions (ICH, EDH, SDH, SAH) the origin of IVH was not determined (MICLG). The most common cause of trauma in this group was motor vehicle accident (2 car collisions, 2 motorcycle accidents and two were hit by motorcycles). And the remaining sequels (3 moderate disability, 2 good recovery and one death) can be related to multifocal intra-parenchymal lesions also known as diffuse brain injury.13, 14, 21 This study showed acute hy-drocephalus as being rare in severe blunt head injury (0.22%) and only 6.45% of patients with traumatic IVH needed ventricular drainage. In LeRoux and colleagues' report only 4 of the 43 patients with traumatic IVH needed ventricular drainage for acute hydrocephalus (93%).8, 22, 23 Desiderio Rodriguas et al. a reported post-traumatic hy-drocephalus (PTH) as a relatively rare but a recognized clinical entity, and their study showed a 2.4% incidence of PTH for both acute PTH and chronic PTH (hydrocepha-lous ex- vacuo) and IVH was the etiology of PTH in 55.4% of the patients.24 CONCLUSION Posttraumatic IVH is a relatively rare but recognized clinical entity. Severity and direction of application of force and other associated abnormalities are major deter-mining factors in the extent of hemorrhage. Acute post-traumatic hydrocephalus is a very rare clinical finding (delayed dilatation of the ventricles after a head injury is commonly due to traumatic cerebral atrophy called hydro-cephalus ex-vacuo)24 and it's presence indicates a very poor prognosis regardless of what treatment methodoloes are taken especially if all four ventricles are filled with blood. This study showed only 3.4 percent of patients with severe head injury developed IVH and 0.22% of them developed acute PTH and only 6.45% of patients with traumatic IVH needed ventricular drainage. REFERENCES
Copyright 2006 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr06004f2.jpg] [mr06004f3.jpg] [mr06004f1.jpg] [mr06004t1.jpg] [mr06004f4.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}