 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
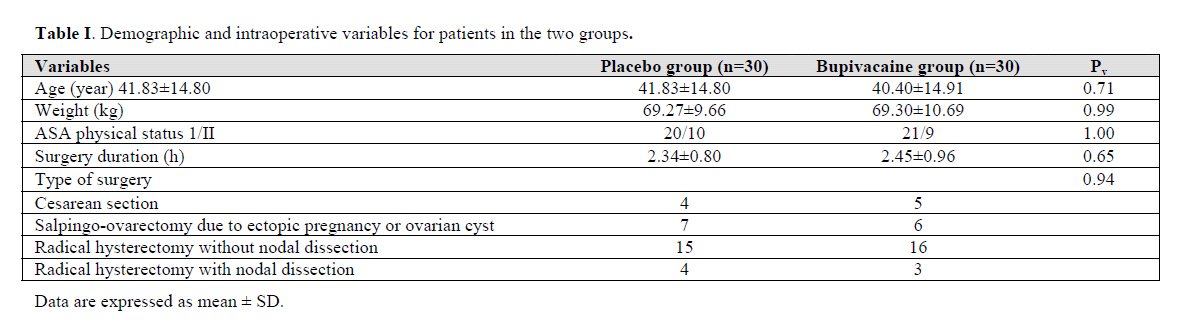
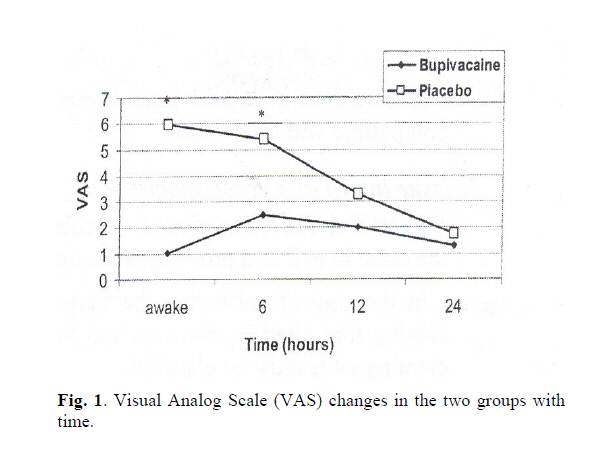
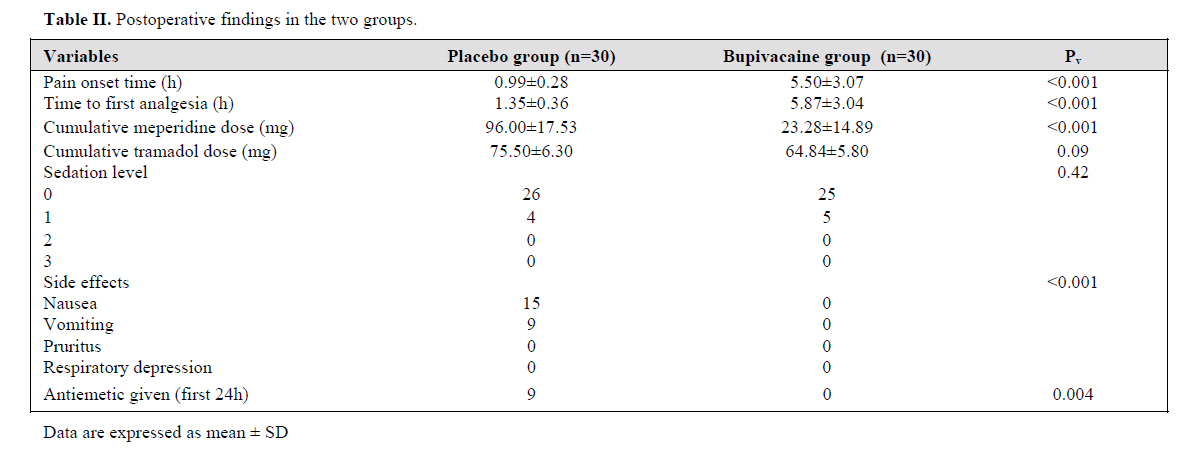
Medical Journal of the Islamic Republic of Iran , Vol. 20, No. 1, May, 2006, pp. 19-22 INTRAPERITONEAL AND INCISIONAL BUPIVACAINE ANALGESIA FOR MAJOR ABDOMINAL/GYNECOLOGIC SURGERY: A PLACEBO-CONTROLLED TRIAL S. ATASHKHOII, M.D., * M. JAFARI SHOBEIRI, M.D., * * AND R. AZARFARIN, M.D.* From the Depts. of *Anesthesiology and **Obstetrics and Gynecology, Tabriz University of Medical Sciences, Tabriz, I.R. Iran. *Assistant Professor of Anesthesiology, Tabriz University of Medical Sciences, Tabriz. Corresponding Author: Dr. Simin Atashkhoii: Iran, Tabriz, South Artesh Ave, aL-Zahra Hospital, Departement of Anesthesia. E-mail: siminatashkhoii@yahoo.com, Tel: 00980914-114-8861 Fax: 0098411-5566449 Code Number: mr06005 ABSTRACT Background: Postoperative pain is an important surgical problem. Recent studies in pain pathophysiology have led to the hypothesis that with periopera-tive administration of analgesics (pre-emptive analgesia) it may be possible to prevent or reduce postoperative pain. This study was planned to investigate the efficacy of pre-emptive analgesia on postoperative pain after major gyneco-logic abdominal surgeries. Keywords: Gynecologic abdominal surgeries, Pre-emptive analgesia, Intraperitoneal infiltration, Bupivacaine INTRODUCTION Postoperative pain management is an important com-ponent of patient care after gynecologic surgery. Analge-sic use strategies in the initial postoperative period com-monly include patient-controlled analgesia, and parenteral nonsteroidal anti-inflammatory agents. These strategies address the problem of pain control only after painful stimuli have been initiated. In contrast, pre-emptive anal-gesia is intervention that is provided before or during op-eration to reduce or prevent subsequent pain.1, 2 Recent studies demonstrated that pre-emptive par-enteral agent use including ketamine,3 ketorolac,4 pro-methazine,5 esmolol6 and meloxicum,7 and regional anal-gesia (with local anesthetics8, 9 or opioids10, 11) reduces pain scores and medication requirements, in many ab-dominal surgeries. The value of locally applied or incisional anesthetics to improve postoperative pain after sur-gery is less certain. Some studies12-17 failed to show a benefit with the application of local anesthetics, while other studies18-29 indicated that pre-emptive intraperitoneal local anesthetics significantly decreased postoperative pain after gynecological laparoscopy or laparotomy. The purpose of this study was to evaluate the analgesic effects of incisional and intraperitoneal bupivacaine after major gynecologic abdominal operations. PATIENTS AND METHODS Sixty ASA physical status I or II, 18-65 year old fe-male patients undergoing gynecologic abdominal surger-ies, were enrolled in this prospective, randomized, double-blind, and placebo-controlled, clinical trial over six months after obtaining written informed consent. Ran-domization process of allocating patients into study groups was performed by forming "randomly permuted blocks" in online software (http://www.Randomization.com). Exclusion criteria were history of severe heart, pulmonary, hepatic, renal or psychological disease, or allergy to local anesthetics. All patients received 5mg oral diazepam 30 minutes before operation. General anesthesia was induced with thiopentone/fentanyl and tracheal intubation. Patients were randomized to receive either 45mL of bupivacaine 0.375% (bupivacaine group, n=30) or 45mL normal saline (placebo group, n=30). Thirty mL and 15 mL of treatment solution were administered into the peritoneal cavity or incision, respectively, before wound closure. Postoperatively, pain intensity was evaluated using VAS (0-10 cm) on awakening and at 6, 12, and 24h. A standard postoperative analgesic regimen was utilized in all patients. The patient was prescribed 0.5 mg/kg meperidine IM as required for analgesia or with VAS ≥4. Sedation level was according to a four-point scale (0=awake and alert; 1=mildly sedated or easily aroused; 2= moderately sedated or can be aroused by shaking; 3= deeply sedated or difficult to arouse, even by shaking). Time to first analgesia request and total analgesic (meperidine and tramadol) requirements at 24h postopera-tively, and side effects such as nausea, vomiting, pruritus, and respiratory depression (yes or no) at 24h postopera-tively were recorded. Statistical analyses were performed using the software package SPSS v12.0 (SPSS. Inc. Chicago. IL). Compari-sons of continuous variables were made using independent t test or Mann-Whitney U test. Analyses of nominal vari-ables were made using χ2 or Fisher's exact test as appro-priate. Repeated measures ANOVA was done to evaluate VAS score changes with time in each study group. The test results were considered significant if p≤ 0.05. RESULTS There was no significant difference in age, weight, ASA class, duration and type of surgery between the pa-tients (Table I). On awakening and 6h after operation, pain scores were significantly less in the bupivacaine group than in the pla-cebo group (p<0.001). However, at 12h (2.03±1.1 v.s 3.271.30; p=0.16), and 24h (1.29±0.9 v.s 1.79±1.0; p=0.31), there were no differences in pain scores between the two groups (Fig. 1). As shown in Fig. 1 the repeated measures ANOVA of VAS score of patients in the bupivacaine group [F (3, 87) =30.18; p=0.0001], and pla-cebo group [F (3, 87) = 276.97; p= 0.0001] revealed that changes with time was significant. Pain onset time and time to first request to analgesia were significantly longer in the bupivacaine patients (5.50 3.07 h, 5.87 3.04 h; respectively) than in the placebo group (0.99 ±0.28 h, 1.35 ±0.36 h; respectively; p< 0.001 for both variables; Table II). The mean meperidine requirement was signifi-cantly smaller in the bupivacaine patients (23.28±14.89 mg) than in the placebo group (96.00±17.53 mg) at 24h postoperatively (p<0.001; Table II). This significant difference was attributable largely to the reduction in meperidine requirements within the first 6h postoperative period. There were no significant differences between the groups in tramadol administration at 24h (p=0.09; Table II). There were no significant differences between the groups in sedation level (p=0.42; Table II). However, there were significant differences regarding postoperative complications such as nausea, vomiting, pruritus and res-piratory depression (p<0.001), and patients who asked for antiemetic (p=0.004) between the two groups at the first 24h after surgery (Table II). DISCUSSION The aim of the present study was to investigate whether infiltration of a local anesthetic solution in the surgical field would reduce the incidence, intensity, and duration of postsurgical pain compared with infiltration of saline in patients undergoing gynecologic laparotomy. A number of previous investigations have examined wound instillation and peritoneal analgesia with local an-esthetics. Some studies were unable to demonstrate a benefit of employing this technique in terms of reduction in the patient's perception of pain.12-17 A qualitative systemic review of the use of incisional local anesthetics for postoperative analgesia after abdominal operations showed that there was improved pain relief after inguinal herniorrhaphy, gynecologic laparoscopy and appendicectomy.18-27 For other types of surgery, such as total abdominal hysterectomy (TAH), open cholecystec-tomy, cesarean delivery, and major upper abdominal surgery, the evidences showing the value of instillation of local anesthetic into the incision are equivocal.12, 17, 28 In the present study, peritoneal combined with subcu-taneously delivery of local anesthetic compared with pla-cebo, beneficial effects were observed. In the treatment group, patients had a better pain score on awakening, and 6h postoperatively, and had a longer interval to first anal-gesia and had reduced opioid requirement in the first 24h postoperatively. The failure of some of the previous trials to show sig-nificant analgesic benefits may be attributed to the site of surgery, timing of the administration, and dose of local anesthetic. In addition it is possible that either incisional or intraperitoneal local anesthetics alone may not be ade-quate to produce measurable postoperative analgesia. Our data suggest that block of both visceral and somatic con-duction is important if an analgesic sparing effect is to be demonstrated after major surgery.27, 28 In the present study, peritoneal combined with subcu-taneously delivery of local anesthetic compared with pla-cebo, beneficial effects were observed. In the treatment group, patients had a better pain score on awakening, and 6h postoperatively, and had a longer interval to first anal-gesia and had reduced opioid requirement in the first 24h postoperatively. This method of delivery of local anesthetic is easy, and no expertise or special training is required. It was not as-sociated with any untoward side effects and did not interfere with the operative procedure. It appears to be a valu- able adjunct to opioids and have an opioid sparing role.25-28 Bupivacaine has been shown to have an analgesic ef-fect beyond the duration of its pharmacological action. It has been postulated that bupivacaine suppresses the for-mation of a hyperexcitable state in the central nervous system which is responsible for the maintenance of post-operative pain.27 No adverse effects are detected from the dose of bupivacaine used in previous studies. This observation is consistent with pharmacokinetic studies in which no ad-verse clinical effects were reported from intraperitoneal bupivacaine. In our study bupivacaine was administered in doses similar to that of these studies and peak plasma con-centrations were much smaller than the generally accepted toxic value of 3 μg/mL.27-29 The dose of bupivacaine used was 150 mg in 45 mL bupivacaine 0.375%, which is lower than the maximum dose (175 mg) of drug for infil-tration anesthesia.1 The benefits of reducing meperidine administration are thought to be related to improved recovery from surgery and anesthesia. In the postoperative period, analgesia, sedation, nausea, and return of bowel motility are impor-tant factors that facilitate recovery.27-29 In this study, the application of intraperitoneal and subcutaneous bupiva-caine was associated with lower pain scores and a reduc-tion in meperidine requirements in the first 24 hours after surgery. Furthermore, there was little nausea and vomiting in the 24 hour period. We conclude that pre-emptive incisional and intraperi-toneal bupivacaine may be recommended because it re-duced pain on awakening and 6h postoperatively, and provided significant supplemental opioid-sparing analgesia for 24 hours after major gynecologic abdominal surgeries. REFERENCES
Copyright 2006 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr06005t1.jpg] [mr06005t2.jpg] [mr06005f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}