 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
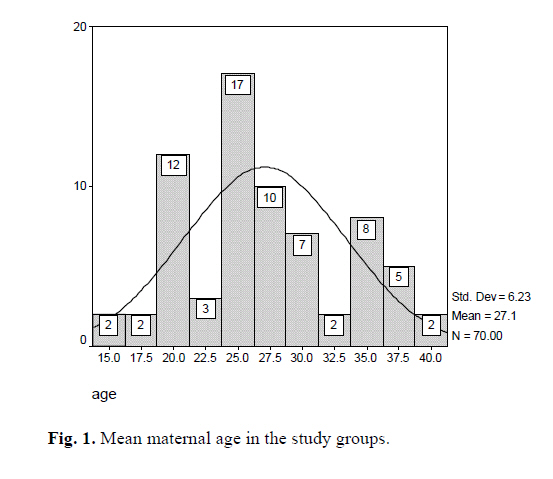
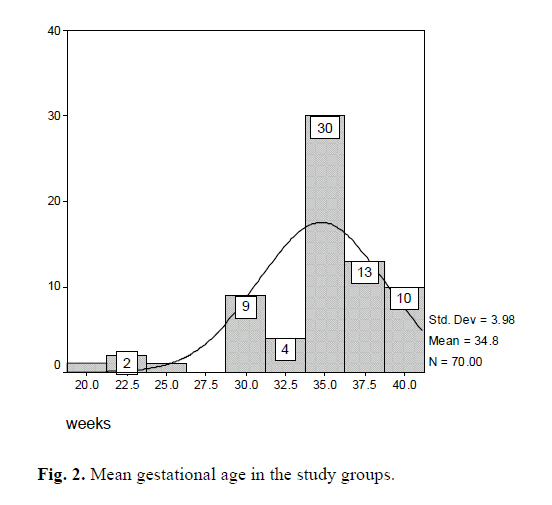
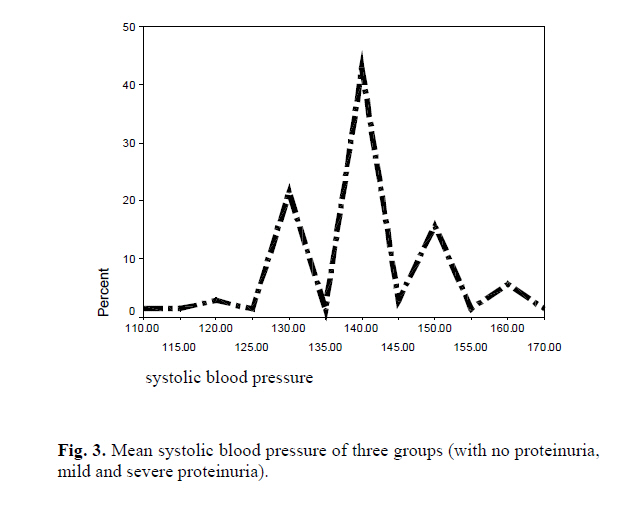
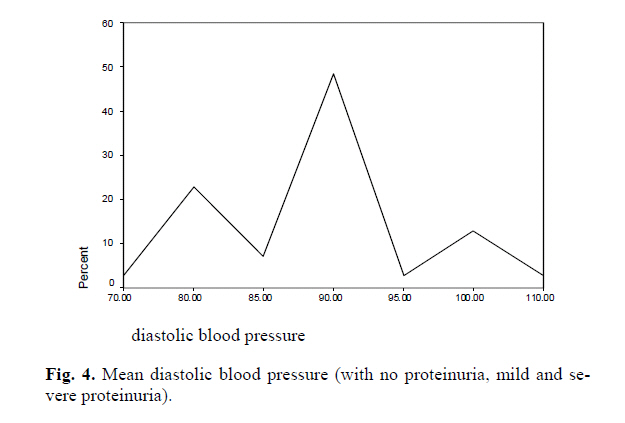
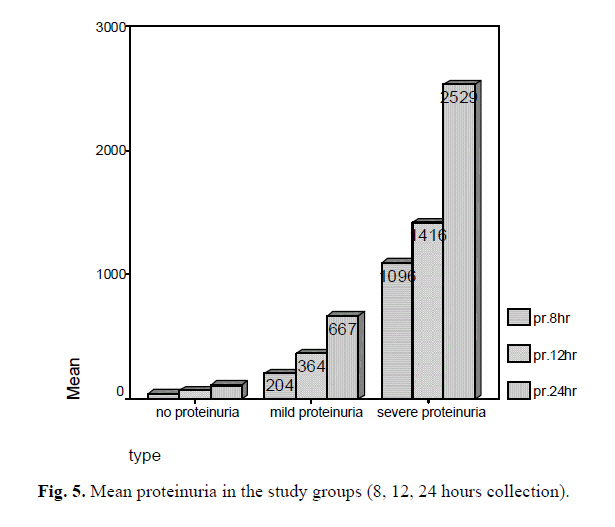
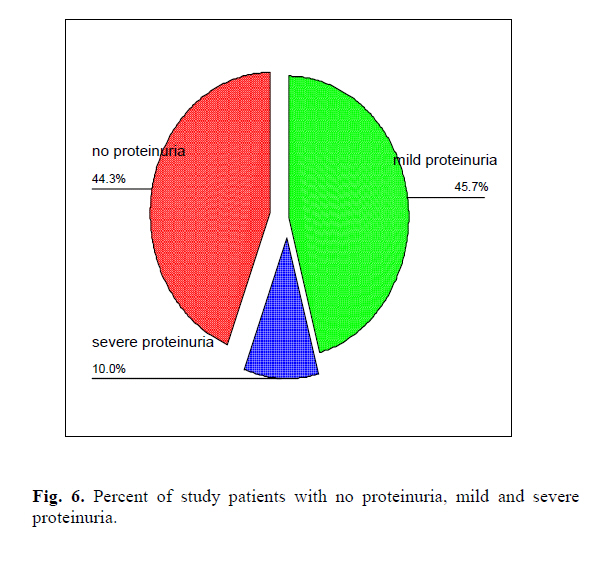
COMPARATIVE EVALUATION OF QUANTITATIVE PROTEIN MEASUREMENTS IN 8-12 AND 24 HOUR URINE SAMPLES FOR DIAGNOSIS OF PRE-ECLAMPSIA M.H. ALAVI AND Z. LAVASANI From the Dept. of Obstetrics and Gynecology, Shahid Akbarabadi Hospital, Iran University of Medical Sciences, Tehran, I.R. Iran. Code Number: mr06006 ABSTRACT Background: In this study our purpose was to determine whether 8 and/or 12 hour urine total protein values correlate with the 24 hour value to confirm the diagnosis of pre-eclampsia. INTRODUCTION Hypertensive disorders complicate 12% to 22% of pregnancies, which account for approximately 15% of pregnancy-related death, represent the second-leading cause of mortality and morbidity. High blood pressure is classified according to preexisting chronic hypertension, pre-eclampsia-eclampsia, superimposed on chronic hyper-tension, and gestational hypertension.1 Pre-eclampsia affects approximately 4.5 to 11.2% of pregnancies in industrialized countries and occurs more commonly in patients at the extremes of the reproductive age range.2 It is seen more often in primigravid women than in multiparous women. Recent epidemiologic studies suggest that multiparous women with different partners have a higher risk for pre-eclampsia than do multiparous women with the same partner3, 4 perhaps because of a pro-tective effect of repeated exposure to specific antigens. Pre-eclampsia affects only pregnant women and is di-agnosed when hypertension and proteinuria occur after 20 weeks' gestation. Edema is often seen but is not required to make the diagnosis. If seizures occur as a complication of pre-eclampsia, the term eclampsia is used. During the past several years, pre-eclampsia-eclampsia has been the second- or third-leading cause of maternal death and is a common cause of fetal morbidity and wastage.5 The diag-nosis of pre-eclampsia is determined by the presence of hypertension accompanied by proteinuria, evident after 20 weeks' gestation. The gold standard for measuring proteinuria is a 24-hour urine sample for total protein, patients with hyperten-sion have only <300mg, those with mild pre-eclampsia have 300mg to 5000mg and those with severe pre-eclampsia have >5000mg of proteinuria.6 The 24-hour period required for collection of the urine results in a delay in diagnosis and treatment or possibly prolonged hospital stay. Shortening the period for diagno-sis of pre-eclampsia would be valuable for management purposes, as well as for decreasing hospital cost and pa-tient inconvenience. A delberg and co-workers showed that total protein values for 6 and 12 hour urine sample correlate positively with values to 24 hour samples for patients with proteinuria. Several investigators have pre-viously reported more rapid methods of identifying pro-teinuria such as the use of protein-creatinine ratios and dipsticks for protein in random urine specimens. These methods have not been shown to correlate with disease severity as determined by the results of 24-hour collection. The objective of this study is to determine if quantita-tive measurements of urine protein from 8- and 12 hour samples as compared to those of 24 hour samples are ac-curate in diagnosing pre-eclampsia and in differentiating it from other disorders. MATERIAL AND METHODS All pregnant patients who were more than 20 weeks gestation who had provided a 24 hour urine sample for protein and creatinine clearance as to rule out pre-eclampsia were included in the study. Participants in the study were inpatients at Shahid Akbarabadi and Firoozgar Hospitals. All of the patients were entered in the study by simple sampling and were excluded from the study if they did not complete the 24 hours of collection because of cesarean-section or vaginal delivery. Total collection time was 24 hours and samples collected in three separate con-tainers. The first container held the 8 hour urine sample, the second container held the next 4 hours of urine and the third container held the remaining 12 hour urine sample. Each container was marked with the patient's name, num-ber of the container, and collection time. The containers were sent to the Shahid Akbarabadi Hospital, where the urine volume in each of the containers was measured separately with a graduated cylinder and recorded. The total 24-hour specimen volume was calcu-lated from the summation of all three containers. The urine was vortexed to ensure homogeneity and a 6 mL aliquot of urine was taken from the first 8 hour collection (# 1). The remaining urine from # 1 was added to the sec-ond container and stirred and 6 mL aliquot was obtained as described for container #1. The first 12 hours of the specimen (#1 and #2) were combined with the 12 hour container (#3), which then represented the urine 24 hour collection. The urine was stirred and a 6 mL aliquot sam-ple was obtained. Analysis for protein in each of the three aliquots was then performed by using a modified Fujita method (Sigma Diagnostic Microprotein-PR Procedure). This assay measures the shift in the absorption that occurs when the pyro-galol red-molybdate complex in the reagent binds basic amino acid groups of protein molecules. The total urinary protein (mg/day) was determined by modifying the total urine volume (mL) by the concentra-tion of protein in the test sample (mg/dL). Creatinine: The urine creatinine was measured by using a modified Jaffe reaction by Sigma Diagnostics. The serum creatinine was determined by using the same assay with 300μL of serum. The creatinine clearance was calcu-lated by using the following formula: Creatinine clearance= Urine creatinine (mg/dL) × vol-ume (mL)/Serum ceratinine (mg/dL) × Time (min) Statistical analysis: Proteinuria from the 24 hour urine result (#3) was categorized into three groups: no proteinuria (<300mg), mild proteinuria (≥300mg to <5g) and severe proteinuria (≥5g). An analysis for variance was used to determine difference in the demographic data. The result of 8 - and 12 hour urine samples were compared to the 24 hour urine results in simple regression analysis to determine a correlation coefficient (r) by using SPSS software. RESULTS There was a total of 70 inpatient hypertensive pregnant women with gestational age more than 30 weeks. Urine specimens were collected at various times throughout the day. Mean maternal age was 27 years (25% under 22, 50% under 26 years and 75% under 31 years), the oldest were 40 years and the youngest were 16 years old. Stan-dard deviation (SD) of maternal age and variance was 6.23 and 38.83 respectively (Fig. 1). Mean gravity and parity of the population were 2.42 and 1.08 respectively; (25% 1, 50% under 2; and 75% under 3 gravity). Standard deviation of gravity and parity were 1.91 and 1.51 and variance of gravity and parity were 3.66 and 2.31 respectively. Mean gestational age was 34.75 weeks (25% under 33.7 weeks, 50% under 35 and 75% under 37 weeks). Standard deviation and variance of gestational age were 3.98 and 15.86 (Fig. 2). Mean systolic blood pressure was 137.78 mm Hg (115-170mm Hg). Standard deviation and variance of sys-tolic blood pressure was 18.3 & 335.24 respectively (Fig. 3). Mean diastolic blood pressure was 88.78 mm Hg (70-110 mm Hg) standard deviation and variance of diastolic blood pressure were 7.77 & 60.46 respectively (Fig. 4). Mean blood creatinine was 0/66 mg/dL (SD and variance was 0.13 and 1.84 respectively). Mean 8 hour urine vol-ume and protein were 479.47 mL and 320.34 mg respec-tively (SD and variance were 317.91 and 151571.1 respec-tively), 50% under 107.5 mg and 75% were under 25 mg. Mean 8 hour creatinine was 328.57 mg/dL. Mean 12 hour urine volume and protein were 821.94 ml and 337.30 mg (SD and variance were 418.43 & 175089.1), 50% of them were under 175 mg and 75% under 434 mg. Mean 12 hour urine creatinine was 558.5 mg. Mean 24 hour urine volume and protein were 1462.94 mL and 605.6 mg respectively (SD and variance were 746.19 & 556811.2 respectively). Mean 24 hour urine creatinine was 1068.94 mg/dL. There was no statistically significant correlation for maternal age with severity of proteinuria (p=0.8, r=0.2), but for systolic and diastolic blood pressure differed weakly (p=0.04, r=0.2). There was no significant differ-ence between the total urine volume, creatinine-clearance, and urine creatinine values between the groups. The 8-hour urine protein results correlated with 24 hour results for patients with mild and severe proteinuria. For detection of C -point by ROC Curve and data from 8, 12, and 24 hour urine analysis, we have no C-Point for the first group and there was no correlation with 24 hour urine sample, but for the second group, values of 70 mg in the 8 hour sample predicted mild proteinuria with a sensitivity of 72%, the positive predictive value was 81% and by using the C-Point of 110 mg, the sensitivity and specific-ity was 81.3 and 81.6 respectively. For the 12-hour sample and the C-Point of 165 mg, sensitivity and specificity was 96.9% and 81.6% respectively. The values for the 12-hour samples correlated significantly with the 24-hour for pa-tients with no proteinuria, mild proteinuria, and severe proteinuria. All patients without disease (first group) had <140mg in 12-hours. For the third group, results of 8-hour samples at the C -Point of 800 with sensitivity and specificity the positive and negative predictive value of 100% (p<0.001, r=1) significantly correlate with 24 hour samples and have a very important statistical value. For the 12-hour samples correlation with the 24-hour samples, in our study we had different C -Point if compared with other studies. All pa-tients with severe proteinuria had values of > 1620 mg in 12 hour samples (Fig. 5, 6). DISCUSSION Pre-eclampsia affects only pregnant women and is di-agnosed when hypertension and proteinuria occur after 20 weeks' gestation. Edema is often seen but is not required to make the diagnosis. If seizures occur as a complication of pre-eclampsia, the term eclampsia is used. During the past several years, pre-eclampsia-eclampsia has been the second- or third-leading cause of maternal death and is a common cause of fetal morbidity and wastage.7 Currently the 24-hour urine is the gold standard for the evaluation of proteinuria.8 A shorter period to diagnosis would have clinical benefits such as shortened time to delivery and earlier use of antenatal glucocorticoids. A more expedient intervention could decrease perinatal morbidity. Certainly those women without pre-eclampsia would be discharged home earlier. If a more rapid and accurate determination of proteinuria was available, this would result in lower length care costs. Patient compli-ance with testing may also improve if the test for proteinu-ria can be simplified or shortened. The quantitation of proteinuria in pre-eclampsia is necessary for diagnosing mild versus severe disease. The results of our study reveal that protein values for the first 8 or 12 hours of a 24 hour urine sampling do cor-relate with the entire 24-hour sample for patients with mild and severe proteinuria. A similar correlation was found between the 12 and 24 hour samples for patients who did not meet the criteria for pre-eclampsia. Therefore it is evident that an 8- or 12- hour urine collection can predict or diagnose mild or severe disease. Total urine protein values of >70 mg in the 8-hour sample or >140 mg in the 12-hour sample were predictive of mild proteinuria. In our study, 8-hour protein values of >800 mg and 12-hour values of >1200 mg were predictive of severe pro-teinuria, however, it should be noted that there were only 7 patients in the severe proteinuria group. Several investigators have explored other means of quantifying proteinuria in a shorter period. The protein- creatinine ratio of a single urine sample from pregnant women has been shown to correlate significantly with a 24-hour collection for patients with protein values of <1g in 24 hours. Above this level the variation between the sample is increased.9 The results of urine dipstick for pro-tein have also been shown by Meyer and co-investigators, to correlate poorly with the 24-hour urine samples for differentiating patients with no disease or severe disease.10 Our study also confirmed that urine dipstick results corre-late poorly with the 24-hour samples. It is speculated that protein excretion varies throughout the day which is thought to be secondary to vasoconstric-tion and vascular spasm producing a fluctuation in protein from moment to moment. Protein excretion tends to in-crease with ambulation and upright body position, which produces renal vasoconstriction and altered permeability of the glomerular barrier.11 These physiologic factors are thought to produce diurnal variation in protein excretion. It is shown that albumin excretion has a circadian rhythm that makes a 24-hour collection necessary.12 The protein excreted in the urine of pre-eclamptic women are hetero-genous and variable and in some cases do not even in-clude albumin. The 8- and 12-hour results collected at different times of the day correlated with the 24-hour val-ues for patients with mild and severe proteinuria. In this study we did not show a significant pattern of diurnal variation in protein excretion. ACKNOWLEDGEMENTS The authors acknowledge the Research Council of Iran University of Medical Sciences for the statistical support. REFERENCES
Copyright 2006 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr06006f2.jpg] [mr06006f1.jpg] [mr06006f4.jpg] [mr06006f6.jpg] [mr06006f5.jpg] [mr06006f3.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}