 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
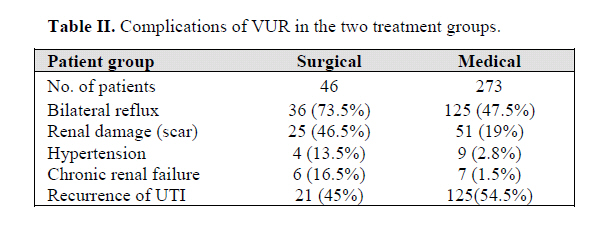
Medical Journal of the Islamic Republic of Iran , Vol. 20, No. 1, May, 2006, pp. 29-32 PRIMARY VESICOURETERAL REFLUX IN IRANIAN CHILDREN:A FOLLOW-UP OF 330 CASES FATEMEH GHANE SHARBAF* * , MOHAMAD HOSEIN FALLAHZADEH**, ALIREZA MODARRESI*, AND MOHAMAD ESMAEILI* From the *Dept. of Pediatrics, Dr. Sheikh Hospital, Mashhad University of Medical Sciences, and the**Dept. of Pediatrics, Nemazee Hospital, Shiraz University of Medical Sciences, Shiraz, I.R. Iran. * Correspondence: F. Ghane, Dr. Sheikh Pediatric Hospital, Tabodi Ave., Mashhad, Iran, Tel: +98-511-7299459, E-mail: ghanefsh@yahoo.com Code Number: mr06007 ABSTRACT Background: Experience with vesicoureteral reflux (VUR) differs in differ-ent centers and there are plenty of controversies. The aim of this study was to evaluate the outcome of primary VUR complications and the rate of recurrence of UTI. Keywords: Vesicoureteral reflux, Urinary tract infection, Complications. Vesicoureteral reflux (VUR) is defined as the backup of urine from the bladder to the ureters and is a risk factor for pyelonephritis. Primary VUR is congenital and is not associated with any underling neuromuscular or obstruc-tive phenomenon.1 Primary VUR is usually detected dur-ing radiological evaluation of children with urinary tract infection (UTI). It can also be identified in the uninfected siblings or offspring of the index patients and with prenatal diagnosis of hydronephrosis. Complications such as renal scarring, chronic renal failure and hypertension are well known in patients with VUR and UTI. Antireflux surgery offers no short-term advantages other than abol-ishing the reflux. It also does not result in improved renal function or renal growth, and does not affect the rate of new scar formation or the incidence of hypertension. To evaluate the outcome of primary VUR, complications and the rate of recurrence of UTI, we reviewed the charts of 330 patients with VUR who were treated and followed at a university center in Mashhad and Shiraz, Iran. PATIENTS AND METHODS The medical charts of all patients with primary VUR dur-ing the last 19 years (1985-2004) in Mashhad and Shiraz were reviewed. Patients with VUR secondary to lower uri-nary tract obstruction, neurogenic bladder, bladder diverticu-lum or nonneurogenic bladder were excluded from the study. Of the 330 children with primary VUR, 319 who had conventional voiding cystourethrograms (VCUG) were included in this study. UTI was defined as positive urine culture, active urinalysis (Pyuria, WBC clump, nitrite) in symptomatic patients. Urine culture was considered posi-tive when two consecutive cultures showed a groth of more than 100,000 colony-forming units/mL of one mi-croorganism in clean-catch midstream specimens in chil-dren with urinary control, and urine collected by sterile bags in those without it. Follow-up urine cultures were done within an interval of 1-3 months or at any time when a fever of unknown origin or urinary symptoms appeared. Positive urine culture in symptom-free cases (asympto-matic bacteriuria) was not considered as UTI. Ultrasono-graphy was performed in all, dimercaptosuccinic acid (DMSA) renal scan in 157 and follow-up VCUG (with a mean interval of 2 years) in 147 cases. DMSA scan per-formed at least 6 months later than acute UTI and renal scarring was defined as an area of photon deficiency or small sized hypofunctioning didney on DMSA or renal parenchymal thinning in ultrasonogram. DMSA scan was not done for all of the cases. Nevertheless this procedure was performed in all cases of high (IV & V) grade VURs. The reason for this pitfall was that many of the parents were concerned about the costs and the adverse effects o radiation. Besides, we did not manage to repeat VCUG in all of the cases, and invasiveness and discomfort of the procedure was the main obstacle. Antireflux surgery was done in 46 (14.7%) of the pa-tients (17 with grade V, 12 with grade IV, 10 with grade III and 7 with grade II). About 93% of the patients re-ceived prophylactic antibiotics (Table I). Statistical analy-sis was done using χ2 and Student's t-tests. RESULTS There were 479 refluxing ureters in 319 patients, and 50% of cases were bilateral. The age at diagnosis ranged from 54 days to 16 years (mean: 4.1 years) and the male-to-female ratio was 0.21 (female=262, male=57) (p=0.002). Follow up duration ranged from 1 month to 16 years (mean: 4.5 years). In 95% of the patients VUR was documented during the investigation for UTI. In 4.5% of the patients a positive family history was the main clue for the investigation. The presenting symptoms of the first episode of UTI comprised of dysuria, enuresis or urinary frequency (30%), fever as the only symptom (35%), poor weight gain (15%), flank or abdominal pain (8.5%) and irri-tability (8%) diarrhea (3.5%). In 90.5% of the patients the isolated microorganism in the first episode of UTI was E. coli. The initial grading of VUR, prophylactic antibiotic ad-ministration and the rate of recurrence of UTI in different grades of reflux are illustrated in Table I. Recurrence of UTI was not statistically significant in different grades of VUR with or without surgery. Ultrasonography of the kidneys and urinary tract was done in all patients and was abnormal in 52.5% (68% with grades V and 55% grade IV, 53% grade III and 32% with grade I and II). The frequent findings in renal ultrasound were caliectasis (n=72), hydronephrosis (n=32), small size kidney (n=30), cortical thinning (n=6). DMSA scan was performed in 157 patients and the findings were in favor of cortical damage in 76 (48.4%) of them. Follow-up VCUG done in 150 (47.9%) of the pa-tients (mean interval: 2.2 years) showed no VUR in 55%, lower grades of VUR in 27.5%, higher grades in 5.5% and no change in 12% of these patients. In 79% of the patients, UTI was treated in the outpatient basis and 21% were ad-mitted to the hospital (repeated admissions were required in 7%). Anti-reflux operation was performed in 7, 10, 13 and 16 patients with VUR of grades II to V, respectively. Open anti-reflux surgery (Cohen surgery) was done for all patients. They had no complications such as urinary ob-struction, etc. after surgery. Complications of reflux and/or UTI, such as chronic renal failure and hypertension occurred in 13 and 13 patients, respectively. In Table II these complications are compared in the two treatment groups. It must be emphasized that 16 patients had renal scarring before the operation and surgical treatment was done for higher grades of VUR (Table I). Renal scarring was detected by sonography in 21 and by DMSA scan in 76 patients. Totally, 76 patients (55 female and 24 male) with renal scars or small hypofunc-tioning kidneys were detected. The frequency of grades (I to IV) of VUR in these patients was 4, 12, 17, 20 and 22, respectively. In 15 patients, the defect was bilateral. In VUR of grades IV and V the frequency of a renal defect was 60% in boys and 37.5% in girls (p=0.006). Taking all grades together, renal scaring was present in 52% of boys and 29% of girls (p=0.001). DISCUSSION Primary VUR is the most common hereditary disorder of the genitourinary tract and is transmitted in an auto-somal dominant fashion.6 The prevalence of VUR in healthy individuals is unknown. Ransley, in a compilation of several publications, reports reflux in 1.3% healthy children.7 primary VUR is found in 29%-50% of children evaluated for UTI.8 VUR is classified into five grades; nondilated ureters in grades I or II, dilated ureters in grade III, and severe dilatation with tortuousity in grades IV and V. The grading of VUR is important because the natural history and the risk of renal damage differs in different grades. Patients with high grade VUR (IV and V) are 4 to 6 times more likely to develop scarring than those with low or moderate (I to III) grade VUR and 8 to 10 times more likely to do so as compared to those without VUR.9, 10 In this study, 21% of the damaged kidneys belonged to the patients with low grades of VUR. It is probable that these lesions are the sequelae of pyelonephritis, as mentioned in Taskinen's study.11 In patients with higher grades of reflux the lesions may be due to both VUR and pyelonephritis or at least in some, associated with congenital defects of the kidney. In one study, severe VUR diagnosed at birth was associated with congenital renal damage and males were affected more often and more severely than females.12 Our results are similar to this report in many aspects, including the frequency of bilateral lesions. In contrast to several previous reports the male to female ratio in our study is surprisingly different.12-15 It is notable that females sig-nificantly out-numbered males in our study; nevertheless kidney scar formation was far more common in the latter group. The pitfall of this conclusion is that DMSA was not performed in all studied cases which could possibly change the results. While the rate of renal damage in the present study was lower than that in some previous reports,16, 17, 18 it was higher than the rate reported in Chinese children (28% of boys and 11% of girls).19 We found that the rate of renal damage in boys was at least 52%. We usually perform DMSA scan in the high risk cases, so some patients with minor defects might have been missed. Despite this fact, the high proportion of renal damage in the boys can be a matter of concern which might be explained by higher grades of VUR. As anticipated, we observed higher rates of renal dam-age in the surgically treated group. This could be due to the fact that surgical intervention was implemented pre-dominantly in higher grades of VUR. In 16 patients the renal scar was documented before the antireflux operation was performed and in 9 patients it was found after sur-gery. All surgically treated patients underwent a repeat DMSA 4 to 6 months after the operation to document new scar formation. We concluded that the renal scar in most of the pa-tients is not related to the surgery per se. Recurrence of UTI was not increased in the higher grades of VUR in contrast to a previous report.20 Recurrence of UTI was not increased in the higher grades of VUR in contrast to a previous report.20 The most common abnormal ultrasonographic finding in the kidneys was caliectasis, followed by hydronephro-sis, small size kidney or cortical thinning that was present in nearly 50% of the patients. In at least one-half of the patients with VUR the initial renal sonography does not predict VUR.21 This was also in keeping with a previous report which show that caliec-tasis or hydronephrosis was the most common predictive sign.22 Although VCUG was not repeated, in some of the low risk patients in whom resolution of the VUR was more predictable, the total number of cure, improvement or spontaneous recovery was more than 80%. This is signifi-cant as compared to the results of other reports.14, 17, 23 We concluded that symptomatic VUR following UTI is more common and less severe in girls and the rate of recurrence of UTI is not directly related to the grade of VUR. Also our study shows that hypertension and renal failure are common complication of VUR, therefore arte-rial blood pressure and renal function need to be continu-ously monitored in these patients (Table II). ACKNOWLEDGEMENT This work has been supported by the Renovascular Re-search Center of Shiraz University of Medical Sciences. REFERENCES
Copyright 2006 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr06007t2.jpg] [mr06007t1.jpg] |
| |||||||||
{kind=link}
{kind=link}