 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Medical Journal of the Islamic Republic of Iran , Vol. 20, No. 1, May, 2006, pp. 37-40 LATERAL INTERNAL SPHINCTEROTOMY UNDER LOCAL ANESTHESIA: A RANDOMIZED CLINICAL TRIAL S. MOHSEN TOWLIAT KASHANI, M.D., * MARZIE LAK, M.D., † HASAN-ALI MOHEBI, M.D., † AND FARZAD PANAHE, M.D. § From the Dept. of Surgery, Baqiyatallah University of Medical Sciences, Vanak
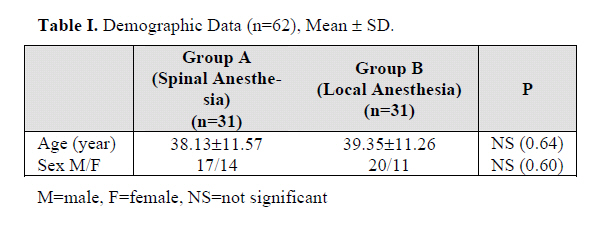
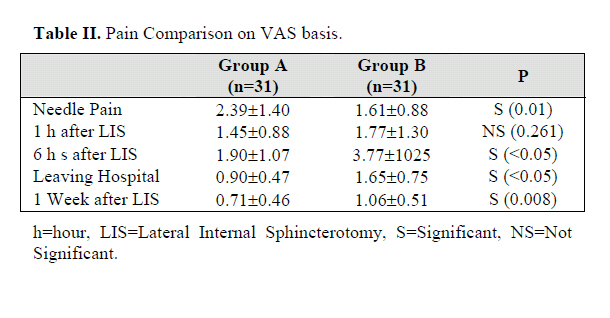
Square, Mollasadra Ave., 19945-587, Tehran, I.R. IRAN. Code Number: mr06009 ABSTRACT Background: Nowadays there is an attempt to perform lateral internal sphincterotomy (LIS) operation on an ambulatory basis under local anesthesia. This study aimed to compare postoperative outcome in local anesthesia with spinal anesthesia. Keywords: Lateral Internal Sphincterotomy, Local Anesthesia, Pain INTRODUCTION An anal fissure is a tear in the bowel lining. It causes painful, bloody bowel movement. It is often confused with hemorrhoids, which are non-painful swellings at the anus caused by enlarged veins. A fissure can be acute or chronic. The chronic condition is often associated with a build up of tissue at the external end of the tear. This is called a sentinel pile and may be noticed by an affected person. Therapy is focused on breaking the cycle of pain, spasm, and ischemia thought responsible for the develop-ment of anal fissure. Medical therapy is an effective method in most acute fis-sures, but will heal only approximately 50 to 60% of chronic fissures.1 Surgical therapy has traditionally been recommended for chronic fissures that have failed medical therapy, and lateral internal sphincterotomy (LIS) is the procedure of choice for most surgeons. Healing is achieved in more than 95% of patients by using this tech-nique and most patients experience immediate pain relief.1 Nevertheless, nowadays there is a tendency to perform anorectal operations on an ambulatory basis.2 In some Hospitals in Italy, recently in Kuanas University Medical Hospital the anorectal procedures especially LIS are car- ried out on a 24-hour stay basis.3 Although organizing an ambulatory center is essential to select patients with re-spect to main and concurrent diseases, selecting the opti-mal anesthesia and home-readiness is significant. Some 20-30 years ago anorectal surgery was regarded as extremely painful. Intensive pain in the operated zone and functional disorder of adjacent organs are distinctive for the postoperative period,4, 5 but today there is an attempt to improve the patient's condition and reduce pain during the ambulatory procedure. However, most surgeons do LIS in the hospital, using general or spinal anesthesia, with the associated high cost of hospitalization.6 In this study we have been searching for a method of treating chronic anal fissure which could be done in an office with less pain and need for opioid usage and subsequently fewer complications. We have modified the method so that we indeed prefer this procedure in the office, using local an-esthesia, as opposed to the hospital and spinal anesthesia. MATERIAL AND METHODS The study was a randomized, double blinded, con-trolled trial. A total of 62 patients aged 15 to 65 with anal fissure complaints were randomly selected for lateral in-ternal sphincterotomy (LIS) in a referral Colorectal Center in Baqiyatallah Hospital between March 2004 and De-cember 2004 in Tehran Iran. The rational for limiting age was the contraindication of using some anesthetic agent in some ages. 31 patients were operated randomly by a sur-geon under local anesthesia (group A) and the remaining were done under spinal anesthesia (group B). We pre-ferred that another surgeon blinded to the anesthetic tech-nique perform the LIS. Only the study statistician and data monitoring physician saw unblinded data and the tech-nique of randomization was based on hospital registration number (even or odd). We emphasized that another sur-geon examine the patients at the same time in a day for pain scale by a 10-cm VAS (Visual Analogue scale) blindly. Also we determined to follow up patients with respect to assessment of their pain simply for 1 week. It seems to us it would be good enough for pain comparison. The chronic anal fissure was described as fissure com-plaints for more than 3 months. Patients with concurrent severe anorectal diseases, any history of allergy sensitivity to anesthetic drugs and who were at high risk for opera-tion according to ASA1 criteria (>III) were excluded. All patients were operated using a uniform method: nothing by mouth 8 hours before operation, no enema and no pre-operative laboratory or manometric study. All had cardiac and pulse oxymeter monitors as well as nasal oxygen 4 to 6 L/min, administered by the surgeon. Medical history and anal examination was first carried out to ensure that no other abnormality is present, and proctoscopy was per-formed in both groups. The preoperative and postopera-tive care was the same for both groups. Informed consent was achieved. In the current study we tested the hypothe-sis that a policy of local anesthesia in LIS would: 1. Re-duce postoperative pain and complications; 2. This tech-nique does not change the rate of satisfaction in comparison with spinal anesthesia. Procedure Before administering a local and spinal anesthetic, the surgeon gave Meperidine 1mg/kg intramuscularly ½ hour before operation for sedation in both groups. In both groups, we preferred to have patients in the lithotomy po-sition. The buttock was retracted and the area was pre-pared and draped. To achieve adequate local anesthesia, a cocktail of local anesthesia, 6cc, composed of 10cc of Lido-caine 2%, an intermediate-acting anesthetic, with 10cc Marcaine 0.5%, a long-acting anesthetic, and the addition of some bicarbonate (0.5cc of 8.4 % sodium bicarbonate [1meq/kg]) was injected into the subcutaneous tissue above and below the anus through a 27-g needle. The ra-tionale for this combination was the rapid effect of Lido-caine and the prolonged effect of Marcaine. However, the rationale for this injection was the sensation of pain under the anorectal dentate line is blocked in these areas. Next, 20cc of the above local anesthetic was injected deep into the inter-sphincteric space on right and left side of the anal canal through a 21-g needle. The index finger of the other hand was inserted into the anal canal and kept there throughout. The surgeon must be completely familiar with the inter-sphincteric groove and be able to feel the distal verge of the internal sphincter with ease. Using this as a landmark, and the index finger guided first the needle and the instrument. In the next group, ½ hours after injection (same the first group), sedation was followed by injection of 50 mg of Lidocaine 5% into the subarachnoid space routinely by the anesthesiologist. Next, the patient was put in a semi-sitting position for 5 minutes to block the saddle nerves. To make precise assessment of these two types of anesthesia, postoperative pain in both groups was assessed by a 10-cm VAS (Visual Analogue scale) in particular on performing the operation. However, for assessing primary outcome, 1 and 6 hours after that and the first week after operation by phone the assessment were done. Data were analyzed by standard statistical methods and the results expressed as mean±standard deviation (SD). Differences between VAS scores were compared using Student’s t-test for unpaired samples; differences between percentages were analyzed using Fisher’s exact test. Probability values of less than 0.05 were considered significant. Analysis of variance was used to compare variables between groups. However, based on 0.9 powers to detect a significant dif-ference, 31 patients were required for each study group. RESULTS Sixty-two patients aged over 15 were studied. None of them were omitted from our study. Patient characteristics are shown in Table I. Male gender was more than female in both groups. There were no significant differences in sex and age between the two groups (p>0.05). There was a significant difference in pain score related to needle pain on performing operation on VAS basis between group A and B (2.39±1.40 vs. 1.61±0.88 ). It indicated that the needle pain of spinal anesthesia was less than local anesthetic injection. To our surprise, a significantly higher VAS score was obtained in the spinal anesthesia group than local anesthesia about 6 hours after the operation, leaving the hospital and at the first week after LIS as shown in Table II. There was no significant difference between both groups in VAS score after 1 hour postoperatively. Patients were asked to grade the results of their operation subjectively as excellent, good and poor. Of the 62 who responded, 90.3% versus 77.4% had excellent result in group A and B respectively. None of them had poor result in both groups. 22.6% in group A claimed they had good result and 9.7% in group B. Nevertheless, there was no significant difference be-tween the two groups (p=0.15). However, our documented data showed that the patients who were performed under local anesthesia with comparison to spinal anesthesia felt a bit more relaxed; there was no significant difference between the two groups. Need of opioid, 24 hours after the operation, in local anesthesia group was significantly less than the other group (28.71±22.17 mg vs. 54.55±22.92 mg p< 0.05). Also patients who underwent LIS under local anesthesia used significantly less Codeine than the other group. (10.4±13.6 mg vs. 18.8±17.8 mg p=0.04). There was a significant difference in postopera-tive gastrointestinal symptoms (nausea and vomiting) in group A in comparison with group B (3.2% vs. 19.4% respectively p< 0.05). DISCUSSION The important note in our study is obtaining adequate anesthesia. The crux of the matter is relief of fissure pain after lateral internal sphincterotomy is immediate. There-after the selection of anesthesia technique is not so impor-tant. However, from approximately 24 years ago, some authorities believed that the aim of any operation is a suc-cessful cure with minimal discomfort and disability to the patient.7 The issue of which technique of anesthesia is best for pain relief has remained a question. It is generally accepted that today the majority of mi-nor anorectal diseases such as chronic anal fissure are performed on an ambulatory basis. Requirements for am-bulatory anesthesia are rapid onset and lack of intraopera-tive and postoperative side effects.2 Regardless of pain comparison in our study, large surveys indicate the inci-dence of cardiac arrest to be from 0.004 to 1 case per 10000 of spinal anesthesia, while hypotension is around 33% and bradycardia around 13% in the non-obstetric population. However, postdural puncture headache is a complication of spinal anesthesia, even though not life-threatening but restricting the activities of daily life and causing hospital admission, while the benefits of local anesthesia, as our study showed, is the minimal incidence of postoperative nausea and vomiting. However, authori-ties believe that it improves postoperative relief.2 Doctor Bell from the University of British Colombia believed that as the experience of the surgeon increases, so does his confidence and ability to perform the lateral internal sphincterotomy under local anesthesia.8 In one study, the author firmly believes that patients with anal fissure are admitted to hospital and should undergo LIS under gen-eral and spinal anesthesia. Postoperative convalescence usually requires two or three days of additional hospitali-zation and 1 week at home. Total loss of time from work approached two weeks in many instances, while patients who were operated under local anesthesia upon late Friday afternoon, recuperated over the weekend and were back to work by Monday morning.9 In our study, we believed that apparently patients who were operated under local anes-thesia will be able to go back to work earlier due to less discomfort and pain. Concerning the importance of different style of surgi-cal treatment of chronic anal fissure, nineteen publications fulfilled the criteria of the study encompassing 3083 pa-tients up to 2002.10 Some authorities believe that perform-ing anorectal surgery under spinal anesthesia requires a trained anesthesiologist and has numerous known compli-cations. On the other hand, local anesthesia can be safely carried out by the surgeon, and has virtually no complica-tion.11 Also, Bupivacaine injection in anorectal surgery may have a role in making patients more comfortable and shorten hospital stay.12 All in all, pain is one of the postoperative complica-tions that requires longer hospital stay in the post anes-thetic care unit.13 Thus it costs more for medical personnel and does not conform to the goal of office-based or ambulatory surgery. Pain after home discharge is correlated with degree of pain after operation. In conclusion the key is to control and suppress pain throughout the recovery period. In this study, local anesthesia is the beneficial solution for reach-ing this goal. CONCLUSION In conclusion, better postoperative pain relief could be accomplished by local anesthesia in ambulatory sur-gery in lateral internal sphincterotomy. The technique helped relax and avoid patient discomfort after the post-operative period. We do not deny the role of anesthetics in day surgery especially in anorectal surgery. They should be experienced in that technique which is of particular importance when dealing with outpatient surgical proce-dures. Nevertheless, we have adopted LIS for the repair of chronic anal fissure as a strictly office or outpatient proce-dure. The post operative pain in this review of our 31 pa-tients was low and patient acceptance has been excellent. REFERENCES
Copyright 2006 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr06009t1.jpg] [mr06009t2.jpg] |
| |||||||||
{kind=link}
{kind=link}