 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Medical Journal of the Islamic Republic of Iran , Vol. 20, No. 1, May, 2006, pp.41-44 HOW TO APPROACH THE PATIENT SUSPECTED OF HAVING ACUTE APPENDICITIS, INTRODUCING NEW CRITERIA: (TWO OUT OF THREE) M.R. KALANTAR MOTAMEDI, M.D., F.A.C.S., * J. KHOSHNEVIS, M.D., † D. NAZEMI, M.D., †M. REZAEI, M.D.,† AND M.R. RADPEY, M.D.* From the Dept. of Surgery, Shohada-e-Tajrish Medical Center, Shahid Beheshti University of Medical Sciences, Tehran, I.R. Iran. * Professor of Trauma and Vascular Surgery, Shohada-e-Tajrish Medical Center, Shahid Beheshli University of Medical Sciences. Code Number: mr07010 ABSTRACT Background: Acute appendicitis is the most common cause of acute surgical abdomen. Inspite of the introduction of ultrasonography, computed tomography scanning and laparo-scopy in the years 1987-1997 the difficulty in accurate diagnosis of acute appendicitis has remained the same. Our way of reaching a decision for operating in a patient suspected of hav-ing acute appendicitis (which will follow) has superiority to other introduced so far approaches.
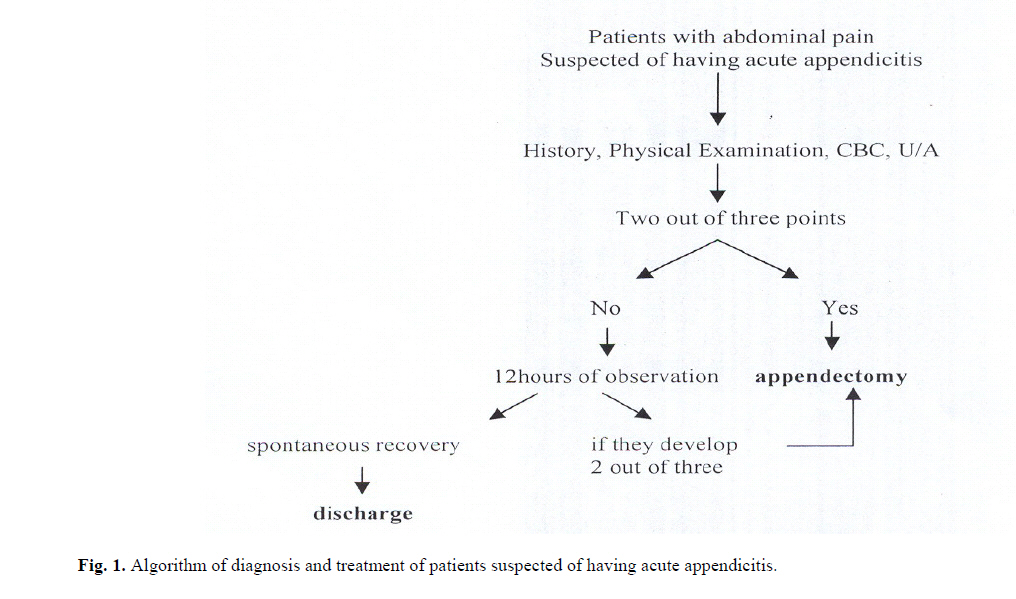
Each of the criteria gets zero or 1 point if it meets that mentioned above and those who get two or three points will be operated on, otherwise the patient will be observed for 12 hours until his symptoms improve or progress to have two or three point criteria when he or she will be operated on. The results of histopathological examination of appendix have been used for the accuracy of this method. Keywords: Acute appendicitis, Diagnostic criteria, Two out of three points (T.O.T). INTRODUCTION Acute appendicitis is the most common cause of acute surgical abdomen.1 The lifetime rate of appendectomy is 12% for men and 25% for women with approximately 7% of all people undergoing appendectomy for acute appendi-citis. The rate of appendectomy for appendicitis has re-mained constant at 10 per 10,000 patients per year. De-spite the high prevalence of acute appendicitis and in-creasing knowledge about the problem, there is still diffi-culty in making an accurate diagnosis of acute appendici-tis and many studies are undertaken all around the world to find new methods, clinical or paraclinical, to increase the accuracy of diagnosis of acute appendicitis1-14 without increasing the rate of perforation. The current accepted accuracy rate in diagnosis of acute appendicitis is around 85%2 and if any center has a negative appendectomy rate of more than 15%, they should revise their approach in making a diagnosis of acute appendicitis. Observing patients suspected of having acute appen-dicitis who do not have typical symptoms can increase the accuracy rate to 94% as reported in some studies. This is associated with an increased rate of ruptured acute appen-dicitis, so delay in diagnosis of acute appendicitis will increase the morbidity rate due to perforation of acute appendicitis.3 In developing countries, limitation for availability of new imaging techniques and trained personnel for its in-terpretation is an added obstacle for making the diagnosis, and dependence solely on clinical findings and simple lab tests are more appropriate. In this study we introduce a new clinical approach to the diagnosis along with laboratory criteria which makes the diagnosis of acute appendicitis more straight forward and with a high accuracy without increasing the rate of perforation, due to delay in making the diagnosis. This is called the rule of two or more out of three. We have performed a research study to evaluate the accuracy of this method at Shohada-e-Tajrish Medical Center, Tehran-Iran, between the years 2002-2005. METHODS A research was carried out to evaluate the accuracy of this method in making the diagnosis of acute appendicitis in a prospective study. During 30 months of study, 3040 patients who were suspected of having acute appendicitis who came to the Emergency Department were evaluated by surgical residents using the rules below for making the diagnosis:
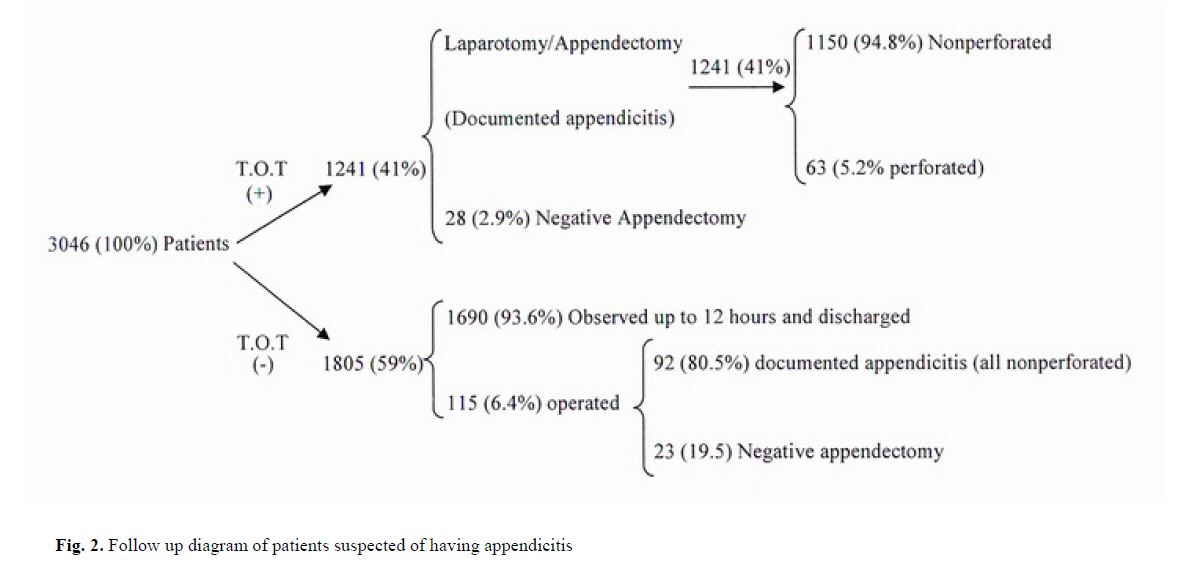
Each of the above gets zero or 1 point and there is not a half point if the criteria is not complete. Patients who get two or three points will be operated on right away, those who do not get 2 out of 3 points will be observed. During the time of observation, if they acquire 2 out of 3 points again they will be operated on right away and if the symptoms improve, the patients will be discharged. RESULTS Among 3046 patients studied 46% were female and 54% were male. Only 2% of patients were under 10 years of age and 35.7% were between 20-30 years old (Table I). Among the males negative appendectomy was higher in both extremes of age but in females, it was more during the reproductive period (20-50 years old); this was statis-tically significant (P<0/05, chi-square). The average age for appendicitis was 25.4 years old both in females and males which is somewhat different with the reported figure in other countries (31.3 years) but the predominance of female over males is the same and statistically significant with P value <0.05. 41% (1241) of patients who presented to the emer-gency department suspected of having acute appendicitis had at least 2 out of 3 criteria and underwent appendec-tomy right away; 97.1% (1213) of these patients had documented acute appendicitis by histopathological re-port, out of these 5.2% (63) had perforated appendicitis which was due to delay in seeking medical attention by the patients or delay in referral of these patients to our center by other medical facilities (the mean time of onset of the pain until the time of arrival to our emergency de-partment was significantly higher in those who had perfo-rated appendicitis). 59% (1805) of the patients who did not acquire at least 2 out of 3 were observed up until acquiring 2 out of 3 points. 6.4%(115) of those who were observed finally acquired at least 2 out of 3 and so were operated on and out of these 80.5% (92) had documented acute appendici-tis and none of them had perforated appendicitis and 19.5% (23) had negative appendectomy. 93.6% (1690) of those who were observed improved and were discharged within less than 12 hours and there was no missed diagnosis of acute appendicitis among these patients during the follow-up (Fig. 2). Overall sensitivity and specificity of this method was calculated at 100% and 97.1%, and the accuracy rate was 98.2% and positive and negative predictive value was 93.3% and 95.5%; the rate of negative appendectomy was only 4.7% which, in comparison with other introduced methods, this method did not cause any perforated appen-dicitis on those who underwent observation. DISCUSSION Despite using advanced technology for making the diagnosis of acute appendicitis prior to surgery in other countries, the rate of negative appendicitis in some reports is still as high as 30-40%.3 While in our study which is based only on history and physical examination and sim-ple CBC, U/A and is practical even in the underdeveloped countries is only 4.7%. Recently a new scoring system for diagnosis of acute appendicitis which was recommended by Alvarado has been published in textbooks. Using this scoring system reported by Alvarado (2005) has decreased the rate of negative appendectomy, while our scoring system with a rate of negative appendectomy of 4.7% is by far superior to the prior scoring systems. The main reasons that clinicians tend to over diagnose acute appendicitis is because of the fear of causing acute appendicitis to perforate while observing the patient sus-pected of having appendicitis. The rate of zero percent of perforated acute appendicitis in those who were observed by us proves that using this point system and observing those patients who do not acquire at least 2 points out of 3 is safe and will encourage clinicians to observe those pa-tients not acquiring 2 points out of 3 with impunity. So our 2 out of 3 scoring system can decrease the rate of negative appendectomy without increasing the rate of perforation of acute appendicitis by observing those pa-tients who do not get at least 2 points out of 3. Teaching this scoring system is very easy and all medi-cal students and interns can become experts in using these criteria for making the diagnosis of acute appendicitis in those suspected of having acute appendicitis and safely observe those who do not acquire at least two out of three. REFERENCES
Copyright 2006 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr06010t1.jpg] [mr06010f2.jpg] [mr06010f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}