 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
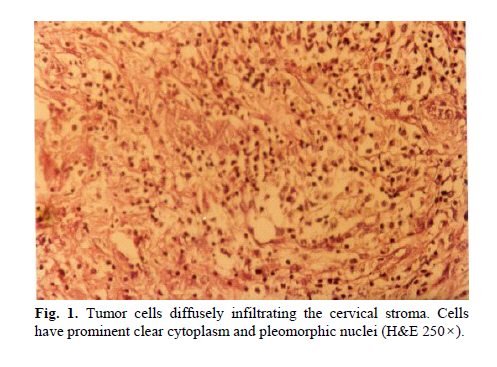
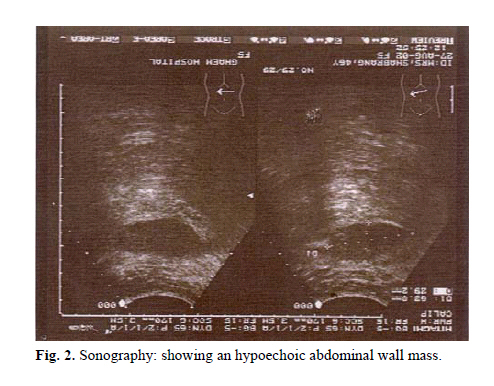
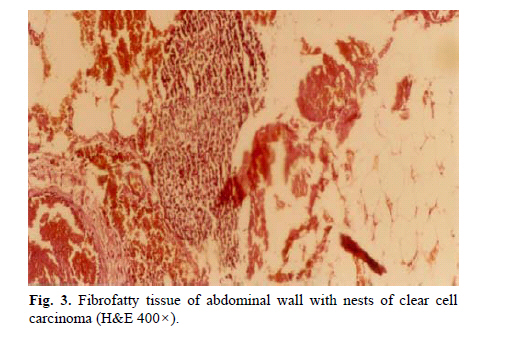
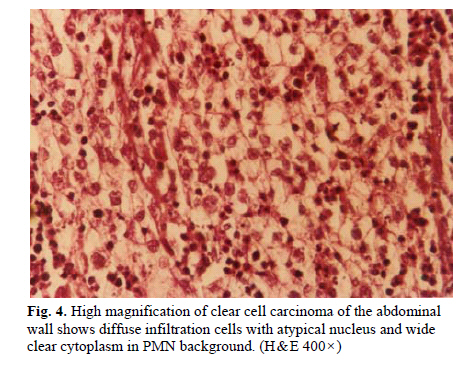
Medical Journal of the Islamic Republic of Iran , Vol. 20, No. 1, May, 2006, pp. 45-47 Case Report ISOLATED METASTASIS OF CERVICAL CANCER TO THE ABDOMINAL WALL Z. YOUSEFI, F. HOMAIE, AND N. SHARIFY From Ghaem Medical Center, Mashhad University, Mashhad, I.R. Iran. * DES: Diethyl stilbestrol. Code Number: mr06011 ABSTRACT Carcinoma of the cervix is a common neoplasm and accounts for a consid-erable number of cervical diseases that lead to death in developing countries. In these countries early detection and improved methods of treatment have re-sulted in comparatively better control of the cancer and long survival; however, invasive and metastatic disease still occurs. The authors present the case report of a 44-year-old woman with clear cell carcinoma of the uterine cervix with metastasis to the abdominal wall. Keywords: Clear cell carcinoma, Uterine cervix, Metastasis of cervical cancer, Neoadjuvant chemother-apy. INTRODUCTION Cervical cancer is spread through direct local and lym-phatic pathways.1 But hematogenous metastasis is rela-tively rare and so is the abdominal metastasis of cervical cancer.2 Clear cell carcinoma (CC) of the cervix and va-gina are identical in development and growth in the area of genital tract which are derived from Mullerian origin.3, 4 Appropriate development can even be traced in young women with vaginal adenosis and in utero exposure to DES * . However, women with no exposure can also be involved.5 In recent years there has been an increasing number of CC affected young females who are in their 20-30s.6 Human papilloma virus (HPV) may be a cofactor in development of CC.7 Mutation in the P53 tumor suppres-sor gene is the second mechanism in the etiology of the rare tumor.8 CASE REPORT A 44-year-old woman para 4 who suffered from ab-normal vaginal bleeding was admitted by a gynecologist. Since she had a polypoid cervical lesion, biopsy was sug-gested and carried out respectively. Postoperative histopathologic diagnosis was clear cell carcinoma of the cervix. A simple hysterectomy was performed in another hospital, and histologic evaluation showed a polypoid tumor with irregular surface approxi-mately 6 cm in size protruding from the cervix correlating with clear cell carcinoma of the uterine cervix (Fig. 1). The patient received external radiation 5040 cGy in 28 fractions and at the end she was treated with only one course of chemotherapy consisting of cisplatin and 5 FU. She didn't return for further cycles. Nineteen months later, she was admitted to the Gynecology Clinic of Ghaem Hospital in Mashhad because of a painful abdominal mass. Initial pelvic examination showed no abnormality and cervical pap smear was reported normal. In abdominal examination there was a tender mass with irregular shape. Previous external radiotherapy caused edema and thick-ness of the abdominal wall. Ultrasonography revealed the existence of an hypoechoic mass (64×29mm) in the right side of the abdominal wall (Fig. 2). Abdominal and pelvic CT scan showed normal other organs. Exploratory laparotomy of the metastasis was car-ried out and revealed an extensive tumoral right abdomi-nal wall and pelvic side wall. Due to wide extension of the tumor, complete resec-tion was not possible. So the patient was treated with ex-ternal radiotherapy with 3000 cGy and she received four cycles of chemotherapy with cisplatin and 5 FU (Fig. 3-4) respectively. At the end of treatment pelvic and abdominal examination were normal in serial follow-up. CT scan, sonography, pap smear and chest X-ray showed satisfac-tory results and no signs of recurrence were observed after 17 months of follow-up. DISCUSSION Cervical carcinoma is the most common carcinoma in young females.9 Clear cell carcinoma of the cervix and vagina in births between 1948-1965 has been frequently seen with in utero exposure to DES.10 A study of 14 cases of CC suggested the etiologic role of HPV as a decisive factor.11 Macroscopically CC is usu-ally an exophytic tumor, while the microscopic appear-ance of the tumor in the vagina, cervix, endometrium and ovary are similar in histologic features.12 Their tissues are composed of large cells with abundant clear cytoplasm and hobnail cells. Several other tumors and tumor-like lesions of the female genital tract may also contain clear cells and may be misinterpreted as CC.13 These misinterpretations usually refer to microglandu-lar hyperplasia, mesonophric hyperplasia. Arias Stella changes, smooth muscle tumor with clear cell, yolk sac tumor, metastatic renal cell carcinoma, signet cell carci-noma and trophoblastic tumor.14 Because of the same his-tologic characteristics mentioned above adenocarcima of the cervix can also have a slightly poorer prognosis than squamous cell carcinoma (SCC) in each stage of the dis-ease.15, 16 Since lymphatic metastasis of these tumors are higher than SCC and so is the grades. Distant metastasis is also more common.16 In a survey of the medical literature the authors encountered different data that reported un-usual distant metastases of cervical cancer to the humerus, psoas19-20 and also abdominal wall metastasis in a few cases.21 However, we had not seen this pattern of metas-tatic clear cell carcinoma before this case. REFERENCES
Copyright 2006 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr06011f4.jpg] [mr06011f3.jpg] [mr06011f1.jpg] [mr06011f2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}