 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
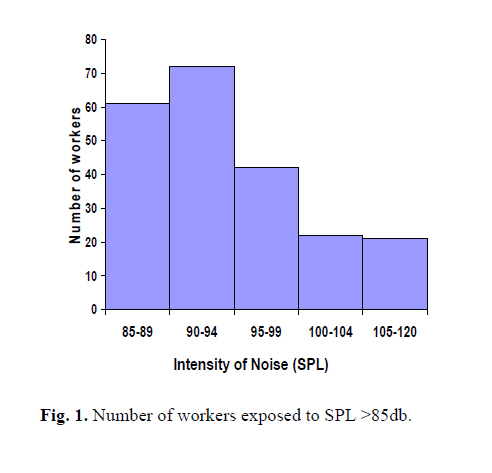
Medical Journal of the Islamic Republic of Iran , Vol. 20, No. 1, May, 2006, pp. 49-51 BRIEF COMMUNICATION PREVALENCE OF NOISE INDUCED HEARING LOSS IN EMPLOYEES IN SHIRAZ INDUSTRIAL FACTORIES A. FARAMARZI, * M. KAVIANI, † AND A. SADEGHI HASSANABADI † * Assistant Professor of Otolaryngology; Department of Otolaryngology, Shiraz University of Medical Sciences. Iran, * Corresponding author: A.Faramarzi, Assistant Professor of Otolar-yngology; Department of Otolaryngology, Shiraz University of Medical Sciences, Shiraz, Iran, E-mail address: Faramarzi@sums.ac.ir, Fax:0098-0711-6279372 Code Number: mr06012 Keywords: Hearing loss, Noise induced, Prevalence Noise-induced hearing loss is the second most com-mon sensorineural hearing loss, after age-related hearing loss (presbycusis).1 Occupational Safety and Health Administration (OSHA) mandates a Hearing Conservation Program if workers are exposed to 85 dB or higher noise levels on a time–weighted average basis for an 8-hour workday. Even limiting noise exposure to 85 dB is estimated to result in hearing loss in 15 percent of exposed workers.2 The most important criterion is that the employee must have been exposed for a sufficient period of time to noise levels loud enough to cause his/her type and degree of hearing loss. The published criteria that support the diag-nosis of occupational hearing loss are as follows:1 signifi-cant exposure to hazardous occupational noise;2 gradual onset of hearing loss;3 symmetrical, or nearly symmetri-cal, hearing loss in both ears;4 hearing loss at approxi-mately 4,000 Hz, commonly referred to as a hearing loss "notch"5 occupational hearing loss is not progressive after a maximum loss in approximately 10 to 12 years after the initial exposure;6 speech discrimination scores are gener-ally not severely affected;7 the maximum amount of hear-ing loss caused by occupational noise exposure to the loudest noises is 40 dB in the speech frequencies and 75 dB in the higher frequencies;8 occupational hearing loss does not progress once the subject is removed from the noisy environment.3 It seems that the prevalence of Noise Induced Hearing Loss (NIHL) or occupational NIHL as the most common oc-cupational disease is high in the developing countries as well. In order to estimate the prevalence of NIHL in workers of industrial factories, after consultation with the occupa-tional health center, five factories where there was more exposure to loud noise were selected. Then interview and physical examination was done in 816 individuals. (March 2002- December 2004) Information collected from the questionnaire included personal data, present and past occupational history, sub-jective estimates of noise exposure, present and past medical history of hearing problems, previous otologic surgery, trauma, otorrhea, hereditary ear diseases, use of ototoxic and other drugs, smoking, hypertension, diabetes, and hobbies. All subjects were examined otoscopically. Pure-tone air conduction audiometric test was conducted to determine the hearing thresholds in the conventional frequencies 0.25, 0.5, 1, 2, 4 and 8 kHz for both ears of each subject, using a Grason-Stadler GSI 16 audiometer, with TDH-5-P ear phone. The audiometer met AN-SIS3.26-1981 standard, and was calibrated in dBHL. Audiometry was performed by an expert audiologist in an ENT university hospital. Noise dosimetry was carried out in all factories by “precision integrating sound level meter” Model 2230 made in Buel & Kjal Company Denmark, by two expert engineers. Only 422 (51%) workers referred to ENT university hospital for audiometry. Ten workers had a history of hy-pertension and 5 suffered from coronary artery disease; Diabetes mellitus was present in five, and four individuals had chronic otitis media. Also 39 female employees worked in offices, so 63 audiograms were omitted from the study. Then 359 audiograms were selected for study of which 241 (67%) belonged to productive workers. Finally data analysis was done by EPIINFO 6. Significance was accepted for all analyses when p<0.05. From the total (816) population of workers, 39 (4.8%) were female and 775 (95.2%) male. The youngest was 18 years old and the oldest 66 years old (average 35.43 years old). The maximum sound pressure level (SPL) to which the workers were exposed to was 120db and the minimum spl was 50 db (average 86.38 and SD=12.29dB). The number of workers who complained from diffi-culty in understanding ordinary speech in the presence of background sound was 57 individuals, with a mean hear-ing threshold of 26.40dB (in frequency 500-8000HZ); the hearing threshold in others without this problem was 18.9dB (p<0.001). About 71 productive workers (29%) complained from tin-nitus with hearing threshold of 22.78dB; the hearing threshold in others without this complaint was 19.46dB (p<0.005). The number of workers with personal sensation of hearing loss was 115 (48%) with hearing threshold of 22.20 dB; the hearing threshold of others without this problem was 18.83dB (p<0.005). About 52 productive workers (22%) complained about poor hearing in telephone conversation with hearing threshold of 24.32dB. Threshold in others without this complaint was 19.42dB (p<0.005). The difference between hearing threshold of workers with other complaints such as nervousness, sleep distur-bance and dizziness was not significant statistically. About the usage of personal hearing protectors, one hundred productive workers (41%) did not use personal hearing protectors because of carelessness (in 84 individu-als), heaviness of earmuff (in 12 individuals), headache (in 3 individuals) and pressure sensation on the auricle (in 1 individual). The combined rate for "all time" and "some-times" users of ear protection devices was about 59 per cent (141 subjects). From the other 141 productive work-ers, 30 subjects (21%) used hearing protection all the time and 211 workers (87 %) sometimes had hearing protec-tion. By multiple range test and Duncan statistical meth-ods, hearing threshold (500-8000Hz) was obtained in two groups of productive workers. The first group were per-sonal hearing protector users and the second group were not. Hearing threshold in the first group was 10.37 dB and in the second 14.04dB (p<0.005). Pure-tone audiometry of the left and right ear in pro-ductive workers showed bilateral and symmetrical, high frequency sensory-neural hearing loss. In this study 482 ears belonged to 241 productive workers. About 218 productive workers were exposed to loud noise equal or above 85db (Fig 1). Hearing threshold in 4000 Hz frequency in the workers within permissible exposure level of ISO was 19.83 db (SD=16.4) and 25.64db (SD=16.24) in the right and left ear, respectively (p<0.05). The number of ears with more than 15 db hearing loss (in frequency 500, 2000Hz) was 60 ears or 12.44 percent of the ears. And the number of ears with more than 30db hearing loss (in frequency 4000-6000) was 30 or 6.22 per-cent of all, so according to the American Academy of Oto-laryngology-Head and Neck Surgery recommendations, they should be referred to an otologist. This finding indicates that the adverse noise effect is generally bilateral and symmetrical, as defined by Alberti (1988) and Ahmed et al. (1999). The occurrence of hear-ing loss as a result of prolonged exposure to a noise level greater than 85 dB (A) without ear protection is well documented in the literature (Berger et al., 1978; Dobbie, 1985; WHO, 1986).4 The present study also found that subjects exposed to daily SPL greater than 85 dB(A) had significantly higher mean thresholds than the nonexposed ones across frequencies tested. The results of this study are in agreement with previ-ous studies that showed noise induced hearing loss pre-dominantly affects frequencies between 4 to 6 kHz.4 The present study found on a group basis (mean thresholds), a maximum hearing loss (dip) localized at 4 kHz, followed by a recovery at 8 kHz. The result of this study in this aspect is in agreement with the conclusion of Ahmed et al.4 Tinnitus is a common symptom of noise overexposure, and it further interferes with hearing acuity, sleep and concentration. These impairments have been associated with social isolation, depression and an increased risk of accidents. In a Canadian series, tinnitus was reported in half the patients applying for compensation, and was independent of age, state of hearing and length of noise exposure.5 But our findings indicated that from all productive workers about 29 percent complained from tinnitus with hearing threshold of 22.78dB; the hearing threshold in others without this complaint was 19.46dB; which was signifi-cant statistically (p<0.005). Although 90 percent of work forces in this study were exposed to dangerous noise more than 85db, there is no active legal support in hearing conservation programs. The results of the present study indicate an alarming start of hearing damage among workers in factories under the study. This warrants a prompt and active application of recognition and protective measure in this regard. According to Suter and Franks, the criteria for pro-grams to conserve hearing are: (a) monitoring exposure to noise, (b) engineering and administrative controls, (c) audiometric evaluation, (d) use of devices to protect hear-ing, (e) education and motivation, (f) record keeping, and (g) evaluating the programme. We also have the same opinion as Malchaire stating that the assessment and pre- vention procedures must be optimised, starting not from the ideal procedure as scientists would see it, but from what industry is willing and able to do.6 Final conclusion is that all industrial factories where noise is above 85dB must implement a hearing conserva-tion program. If hearing conservation is to be improved then senior management as well as the workforce needs to be educated and motivated, and the otolologist's roles are: 1) Supervision of the hearing conservation program, 2) Review of the abnormal audiograms, 3) Detection of high risk individuals, 4) Education about how the hearing sys-tem works, and how noise destroys that, 5) Explanation of preventive measures, and 6) Advising the program admin-istrator. Also the role of active legal support in hearing conservation programs is significant. REFERENCES
Copyright 2006 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr06012f1.jpg] |
| |||||||||
{kind=link}