 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
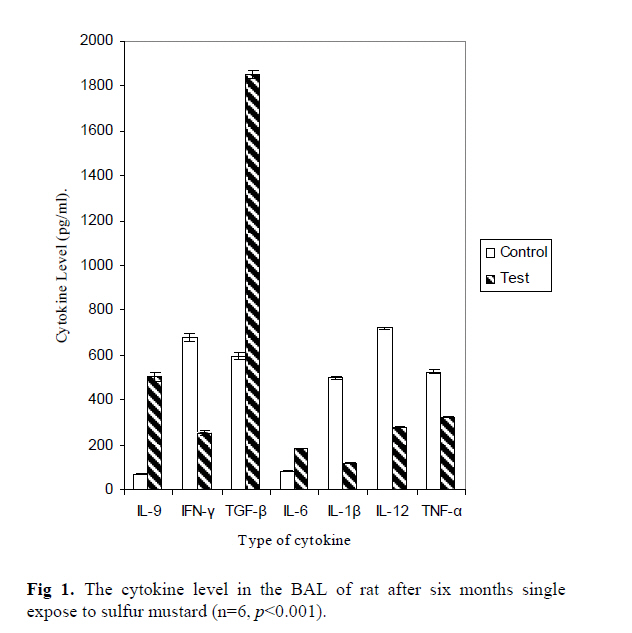
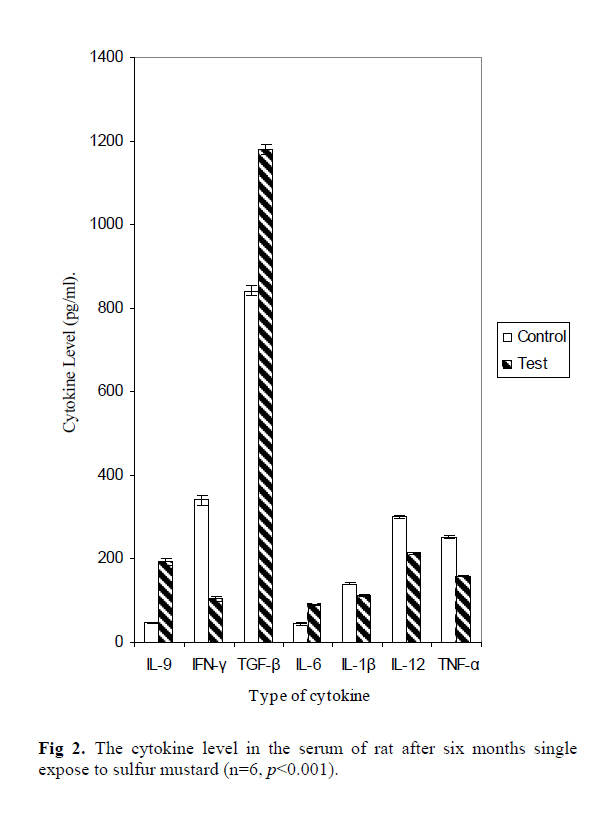
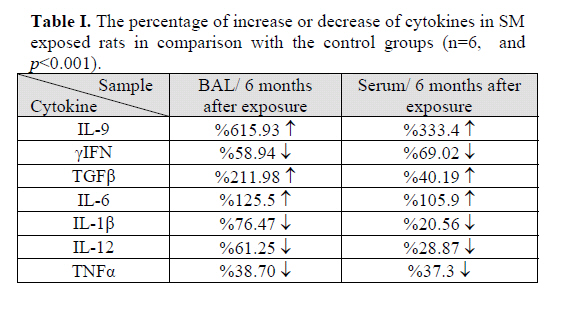
Medical Journal of the Islamic Republic of Iran , Vol. 20, No. 2, July, 2006, pp. 52-56 CYTOKINE PATTERN IN SERA AND BRONCHO-ALVEOLAR LAVAGE SIX MONTHS AFTER SINGLE EXPOSURE TO SULFUR MUSTARD * KAZEM AHMADI, Ph.D., AND GHASEM SOLGUE, M.Sc.** From the* Department of Immunology, Faculty of Medicine and Research Center of Molecular Biology, and the ** Research Center of the Chemically Injured, Baqiyatallah University of Medical Sciences, Tehran, I.R. Iran. Code Number: mr06013 ABSTRACT Background: Cytokines play a major role in both acute and chronic inflammatory processes, including those produced by Sulfur Mustard. This study describes the cytokine level six months after exposure to a single dose of sulfur mustard, defined by IL-1β, IL-6, IL-9, IL-12, TGFβ and TNF-α. Keywords: Sulfur Mustard, BAL, Cytokine, Serum, IL-1β, IL-6, IL-9, IL-12, TGFβ and TNF-α. INTRODUCTION Based on the cytokine environment present in Interstitial Lung Diseases (ILDs) and the pattern of gene expression of unfractionated Broncho-Alveolar Lavage (BAL) cells from ILD patients with lung inflammation, it appears that the macrophages in lung disease have undergone alternative, rather than classical, activation.1 Recent studies have added to our understanding of the role of cytokine and cytokine receptors in the generation of pulmonary inflammatory responses. In the lung, the production of cytokine and expression of cytokine receptors is under complex biologic control, including negative and positive feedback by the cytokines themselves.2 IL-9 is a multifunctional cytokine produced by activated Th2 cells that promotes inflammation and air-way hyperresponses.3 IFN-γ is a key factor in the events that favour local immune responses in the lung. It activates pulmonary macrophages to phagocytose pathogens. IFN-γ is typically expressed by Th1 cells infiltrating the lung in most ILDs.4 IL-1β is produced by alveolar macrophages in response to several inflammatory stimuli in various ILDs.5 Since IL-1β promotes the proliferation of fibroblast and increased collagen production, it has been involved in the development of lung fibrosis associated with ILDs. In the lung, IL-6 is mostly produced by alveolar macrophages. An increased release of IL-6 has been involved in the pathogenesis of various ILDs.6 IL-12 is mainly produced in the lung by macrophages and dendritic cells. In synergy with IL-15, IL-12 favours the contact between activated T cells and antigen presenting cells (APC).7 TGF-β is a potent immunosuppressive molecule that exerts chemotactic effects on monocytes. It modulates the synthesis and the effect of several molecules, including IL-1, IL-2, IL-3, GM-CSF, IFN-γ and TNF-α. TGF-β, which is constitutively released in the respiratory tract, is involved in the pathogenesis of fibrotic processes associated with most ILDs.8 In the lung of patients with ILDs, TNF-αstimulates and regulates the synthesis and release of other lymphokines such as IL-1, GM-CSF, Platelet-activating factor, IL-6 and increases prostaglandin (PG) E2 production9 . Sulfur Mustard (SM) induced cytotoxicity is due to the alkylation of a critical intracellular target, thereby interrupting the control of normal cellular processes.10 Recent studies have, nevertheless, reported characteristic clinical and immune responses to SM, which include a unique case definition of pulmonary damage and cytokine production.11-16 SM exposure produces a chronic immunocompromised condition, which systemically induces abnormal serum levels of Th1 and Th2 cytokines.17-19 Few studies have been carried out on in vitro models of respiratory epithelial cells, which represent one of the main targets of SM.20-22 A study on the effects of SM on tracheal epithelial cells has shown that mild doses of SM induce apoptosis, while higher doses induce necrosis.23 Evidence of an increased death toll from respiratory diseases and a higher incidence of chronic bronchitis have been reported in Japanese workers .24 Manning et al.25 found that pneumonia was the only cause of increased mortality among British SM factory workers. In vitro studies on human mononuclear leukocytes have demonstrated SM-induced mononuclear leukocyte cell death in a time-dependent fashion26. In a separate study Lardot et al.27 demonstrated that SM exposure can modify the expression by cultured human keratinocytes of interleukin-8. They observed a significant increase in the amount of IL-8 secretion by human keratinocyte treated with 1×10-3 M SM after 6 hours of exposure. They have also demonstrated that treatment with 1×10-6 M and 1×10-5M SM, induced no significant differences compared with the control group.27 On account of the high incidence of debilitating exposure to SM during the Iran-Iraq war, there is an increased interest in its mechanism of action and in the development of therapeutic interventions to prevent SMinduced lesions. The aim of this study was to investigate whether SM affects cytokine production by macrophages involved in lung inflammation. PATIENTS AND METHODSAnimals Twenty-four male rats, aged 8 weeks old and weighing 150 g, were divided into two twelve-member groups: control and test. The animals were maintained in dust-free bedding cages in the animal unit. The twelve animals in the test group were exposed to the vapours of SM (obtained from The Ministry of Defence) through inhalation (42.3 mg/m3)28 for 30 minutes in a small cage. The animals in the control group were exposed to acetone only. During each two months, two animals were examined for lung damage29. Based on no clear damage to the lung after 2 and 4 months of exposure and death of two animals by six months29, the experiment was terminated at six months for cytokine assay in the remaining 6 animals of each group. Serum Samples After the animals had been anesthetised, blood samples were obtained from their heart using 5-mL syringes. The blood samples were centrifuged at 1500 rpm for 10 minutes, and sera were separated and kept at -20ºC until they had been analysed for cytokine assay using the ELISA kit (Bender Med Systems, USA). Broncho Alveolar Lavage (BAL)The animals having been anesthetised, their BAL was obtained by cannulating the trachea and lavaging the lung six times with a single volume of 15 mL of ice-cold sterile NaCl 0.9%. This BAL fluid (BALF) was centrifuged (1.000 ×g) for 10 minutes at 4ºC. The free cells BAL fluid was kept at -20ºC until it had been analysed for cytokine assay using the ELISA kit (Bender Med Systems, USA). All cytokine assays was performed in molecular immunology laboratory in Baqiyatallah Medical Sciences University. Statistical AnalysisAll experiments were performed six times (n=6) and the data were analysed by Mynova software using t-test. RESULTSThe results showed significant differences (p<0.001) between the control and exposed groups in terms of all cytokine (IL-9, γIFN, TGFβ, IL-6, IL-1β, IL-12 and TNFα) productions in both the BAL fluid and serum (Fig. 1,2). The most noticeable enhancement in cytokine release was seen in IL-9, which was 615.93% and 321.88% for the BAL fluid and serum, respectively (p<0.001). After IL-9 the highest increase was demonstrated for TGF-βand IL-6 in the BAL fluid which was 200.85% and 125.50% respectively. In both BAL and sera, a significant reduction was seen by γIFN (58.95% and 69.02% for BAL and sera respectively). The rate of reduction for IL-1β, IL-12, and TNF-α in the BAL was more than that in sera, but no significant difference was seen in the rate of TNF-α reduction in BAL and sera (Table I). DISCUSSIONThe reactivity of cytotoxic alkylating agents with DNA, RNA and proteins can cause mutagenic damage and cell death.30 Moreover, the underlying immunological effects of SM exposure have remained poorly defined. Recent studies, however, have reported clinical and immune responses to SM, which include a unique case definition of pulmonary damage and cytokine production. Previous studies indicate that SM exposure produces a chronic immunocompromised condition, which systemically induces abnormal serum level of Th1 and Th2 cytokines.17 Since infiltration by lymphocytes and polymorphonuclear leukocytes represents one of the first events observed in vivo upon exposure to SM, this study examined whether SM exposure could modify the production of cytokines. The results of this study showed that SM inhalation up-regulated IL-6, IL-9 and TGF-β release in the BAL fluid and serum and down-regulated IFN-γ, IL-1β, IL-12, and TNF-α (p<0.001), indicating the possible role of cytokines in lung inflammation in chemical warfare victims. In our study, a high level of IL-9, TGF-β and IL-6 were demonstrated; indicating the possible effect of SM induced lung injury via these above mentioned cytokines. Supporting our view, Arrovo et al.12 reported an increase in IL-1β, IL-6 and TNF-α release by human epidermal keratinocytes exposed to SM, demonstrating the important role of these cytokines in SM injury. In favour to our findings important roles for TNF-α, TGF-β in lung inflammation have been established by other researchers 31, 32 Aghanouri et al.33 reported a significant difference in the level of TGF-βbetween chemical warfare victims and control group, proposed that IFN-γ could be a useful drug for those suffering from lung inflammation. Hassan et al. 34 in a recent investigation demonstrated that SM caused an overall suppression of the immune response. There is also ample information demonstrating the role of IL-9, IL-12 and IFN-γ in promoting lung injury. 35, 36 In this study, the level of TGF-β and IL-9 were increased, while IFN-γ showed a significant reduction (p<0.001). Therefore it seems that macrophages by enhancing the IL9 production are trying to act in opposite action of TGF-β. Related to our results, Gary et al.36 demonstrated that IL-9 has the capacity to modulate the development of lung fibrosis. Noticeable changing in the level of cytokine after six months exposure to SM in this study, show that SM may induce an alteration in gene expression which are primarily involved in inflammation, apoptosis and cell cycle regulation.37-40 Related to our view, microarray analysis provided the opportunity to identify multiple transcriptional biomarkers associated with SM exposure.41 Rogers 41 demonstrated that in an SM-exposed skin, a total of 19 genes within apoptosis, transcription factors, cell cycle, inflammation, oncogens and tumor suppressors categories have been up-regulated. In conclusion, in light of the results of this study and other similar investigations, it seems that SM, by modulating macrophage function in terms of the production of inflammatory cytokines, might be responsible for lung inflammation. The results of this study also provide a further understanding of the molecular responses to inhalation SM exposure, and enable the identification of potential diagnostic markers and therapeutic targets for treating SM injury. ACKNOWLEDGEMENTSThanks are due to The Research Center of the Chemically Injured for financial assistance. This project was approved by the vice chancellor of research of Baqiyatallah Medical Sciences University. REFERENCES
Copyright 2006 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr06013f2.jpg] [mr06013f1.jpg] [mr06013t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}