 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
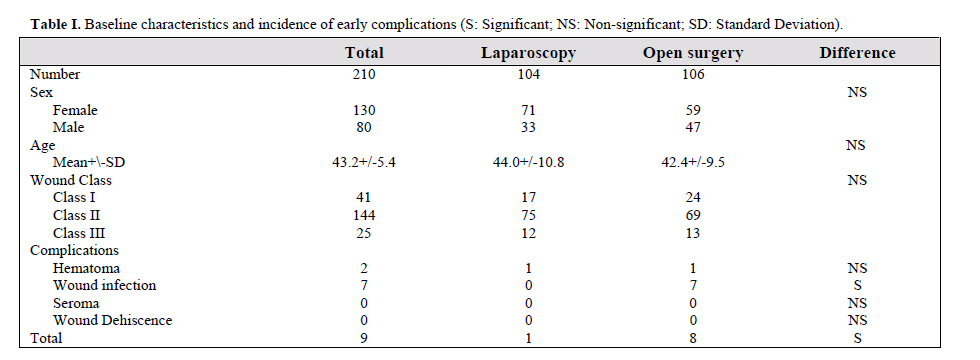
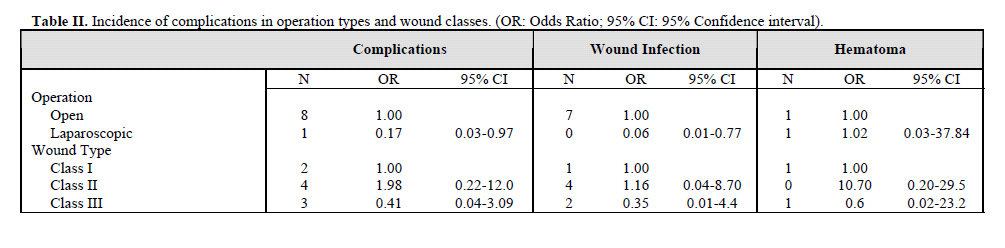
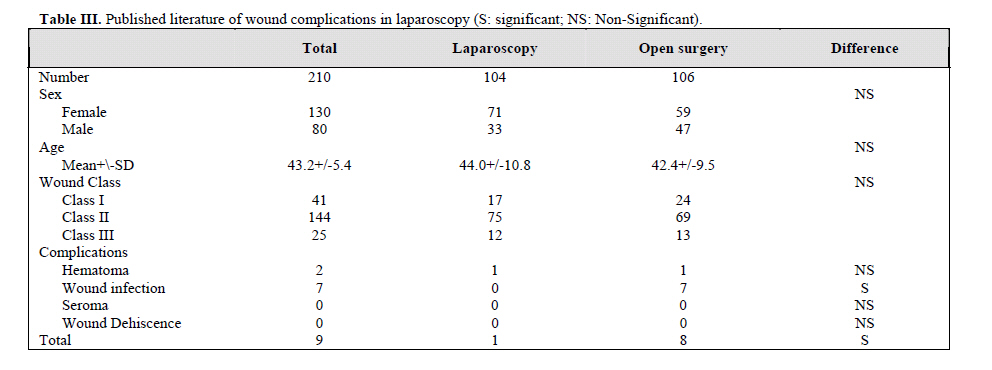
Medical Journal of the Islamic Republic of Iran , Vol. 20, No. 2, July, 2006, pp. 58-61 REDUCED INCIDENCE OF EARLY COMPLICATIONS OFSURGICAL WOUNDS IN LAPAROSCOPIC SURGERY B. KHORASANI, MD *, AND A. GHOLIZADEH PASHA, MD† From the University of Social Welfare and Rehabilitation Sciences, Tehran, and Babol University of Medical Sciences. Babol, Iran. Code Number: mr06014 ABSTRACTBackground: The incidence of early wound related complications is assessed in laparoscopic versus open abdominal surgeries. Complications of surgical wounds (esp. wound infections) are considered as a major problem in surgery wards. Complications of surgical wounds are classified as early and late. Common and early complications are hematoma, seroma and wound infection. Keywords: Wound Complications, Laparoscopic Surgery, Open Surgery. INTRODUCTION Minimally invasive procedures have faced wide acceptance because of smaller incision, less postoperative pain, less ileus, lower rates of pulmonary complications, and most of all shorter hospital stay and quicker return to activities of daily living. 1-5 This clinical trial has aimed to assess the incidence of early wound related complications including hematoma, seroma, wound infection, and wound dehiscence in laparoscopic versus open abdominal surgeries performed in our center. MATERIALS AND METHODS From June 2002 to January 2005 data from medical records of 104 elective laparoscopic surgeries performed by the author at Milad Hospital, were prospectively reviewed. Operations studied included laparoscopic appendectomy, cholecystectomy, ventral hernia repair, and bariatric surgery. To provide a comparable reference,106 diagnosis matched open procedures over the same period were selected and evaluated. Patients above 60 or those with underlying diseases including heart failure, diagnosed COPD, chronic liver diseases, diabetes, and those having taken steroid drugs or having a history of chemotherapy or radiotherapy were excluded from the study. Surgical operations lasting for more than 2 hours and wounds found to be dirty during the operation were also excluded. All the operations were performed under general anesthesia by the same surgeon. Study data included patients` sex, age, wound class, type of operation, and occurrence of early wound related complications. Surgical wounds were classified based on the presumed magnitude of the bacterial load at the time of surgery6. Class I included clean wounds with no infection, class II included clean / contaminated wounds, in which a hollow viscus with indigenous bacterial flora was opened under controlled circumstances, and class III wounds included contaminated wounds with extensive introduction of bacterial flora. Surgical wounds were evaluated for presence of early complications during the post-op hospital stay, and reexamined 10 to 15 days after the operation in the ward or on the first follow up visit in the clinic. Wound infection was defined as painful erythema or culture proven wound drainage, necessitating either antibiotic administration or local wound care intervention. Comparisons were made using a chi-square or student t-test, each when indicated. Odds ratios were calculated using 95% confidence intervals of limit. A P value of less than 0.05 was considered as a significant statistical difference. RESULTS210 patients, including 130 females and 80 males, with mean age of 43.2 years (range 17-60) (Table I) were studied. There were no significant age and gender differences between the two operation groups. Classification of surgical wounds included 41 class I, 144 class II, and 25 class III wounds. The two groups were not different regarding wound classes either. Wound related complications occurred in 9 patients; 2 patients had hematoma and 7 developed wound infection. There were no cases of seroma or wound dehiscence. Incidence of hematoma was similar in the two groups. One patient in laparoscopic surgery (hernia repair) and one in the open operation group developed hematoma. All 7 cases of wound infection occurred in the open method, 1 with wound class I, 4 with class II, and 2 with class III. Risks of developing wound complications in operative methods and wound classes are presented in terms of odds ratio in Table II. Laparoscopy significantly reduced the risk of wound infection and early wound complications in general, but not hematoma. Gender, age, and wound classes were not associated with higher rates of any of the wound related complications. In order to determine the independent effect of operation method on the complications, comparisons of the operative methods were performed within each wound class, which showed reduced risk of wound infection with laparoscopic surgery. DISCUSSION Wound related complications are a great source of trouble in the post-op period; they slow down the wound healing process, lengthen the hospital stay, and their treatment imposes large costs to the health services.7,8 In this study laparoscopic surgery significantly reduced the incidence of early wound complications (0.01% vs. 0.08%; OR (95%CI):0.17 (0.03-0.97)). This was in concordance with previous studies. 2,4,9 Despite the expected lower incidence of hematoma with laparoscopy as a result of minimal tissue damage, one case of hematoma occurred following an inguinal hernia repair. This may be explained by the presence of enriched blood vessels and lymphatics in the region.10,11 The risk reduction effect of laparoscopy on wound infection was remarkable (OR95%CI):0.06(0.01-0.77)). Risk of wound infection in laparoscopic procedures has been so little that some studies have debated the necessity of antibiotic prophylaxis before basic laparoscopic surgeries12,13. The most favorable results of laparoscopic methods in reducing infection has been reported with ventral hernia repairs (3% vs. 22%).2 Wound infection incidence has also decreased following laparoscopic cholecystectomy (2.3% vs. 6.3%) 9, appendectomy 14 and colorectal surgeries (0% vs. 9.5%). 15 Although one study has reported higher infection rates with laparoscopic colectomy (13.5% vs.10.9%), 10.8% of infections in this study has been in the extraction site, and only 2.7% in the trocar site16. For easy comparison, wound infection incidence rates among laparoscopic surgeries as well as open methods have been summarized in Table III. Although laparoscopy has been outstanding in most digestive surgeries, its advocation in more complex surgeries and those for cancer requires developing of well-established operative techniques and equipment in order to ensure patient safety and excellent outcomes. REFERENCES
Copyright 2006 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr06014t3.jpg] [mr06014t2.jpg] [mr06014t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}