 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Medical Journal of the Islamic Republic of Iran , Vol. 20, No. 2, July, 2006, pp. 66-68 EVALUATION OF THE RESULTS OF SURGICAL AND MEDICALTREATMENT IN 16 PATIENTS WITH VERTIGO SECONDARY TOCERVICAL SPONDYLOSIS M. MAZLOUMI, MD*, AND F. SAMINI, MD† From the Department of Orthopedic Surgery, Ghaem Medical Center, Mashhad Medical University, Mashhad, Iran. Code Number: mr06016 ABSTRACT
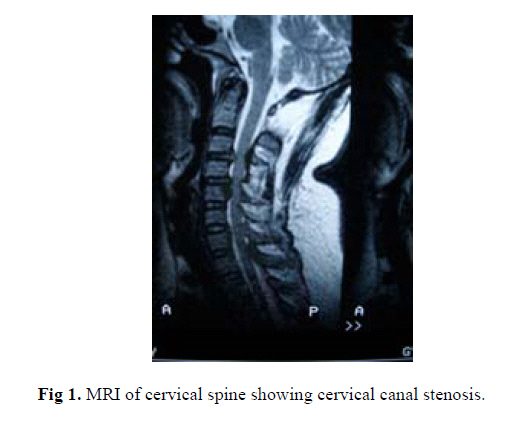
Background: In patients with cervical spondylosis, cord compression and impingement of cord vessels as well as the vertebral artery may be accompanied by vertigo. We evaluated improvement of vertigo in these patients after surgical and medical treatment. Keywords: Cervical spondylosis, Vertigo, Cord compression, Vertebrobasilar insufficiency, neurovascular decompression, Foraminotomy, Laminectomy. INTRODUCTION Cervical spondylosis is a common age-related change in the area of the cervical spine which can cause vertigo. The degenerative changes can alter the alignment and stability of the spine. Cervical spondylosis may be without symptoms or may produce symptoms related to pressure on the cord and associated nerves and blood vessels. By the age of 50, 25-50% of people develop cervical spondylosis. by the age of 75 years, it would be present in at least 70% of people.1 Vertebral artery stenosis resulting from spur formation in the transverse foramen or thromboembolic change in the artery can cause vertigo, especially in old patients.2,3 To evaluate rotational vertebral artery occlusion in the patient with severe cervical spondylosis, Angiography and Doppler Sonography and three-dimensional CT are useful screening modalities. 4,5,6 The aim of this study was to review the effects of surgery and medical treatment in patients with vertigo secondary to cervical spondylosis. PATIENTS AND METHODSIn this study we reviewed prospectively sixteen consecutive patients with vertigo and cervical spondylosis between 1999 and 2004. There were ten males and six females. After complete evaluation of patients with clinical examination and imaging studies of the cervical spine consisting of plain X-ray and MRI, diagnosis of cervical spondylosis and cervical canal stenosis and other pathologies were confirmed ( Fig. 1). All patients had vertigo, and ENT and neurologic examination had excluded causes relating to respective fields. In patients with vertigo after rotation of the neck, for identification of vertebral artery occlusion, we performed Doppler Sonography. Chart reviews were performed with special attention to preoperative patient's age, duration of symptoms, ambulation status, and analgesic use. In seven patients with cervical canal stenosis we performed laminectomy and foraminotomy and resected the osteophytes. In two cases resection of one or two transverse processes through an anterior approach with drilling of the spondylotic spurs of the uncinate processes were performed to decompress the vertebral artery. Two patients with vertebral artery stenosis had angioplasty and cervical orthosis thereafter and seven patients followed a program of physical therapy with cervical traction and muscle exercises and collar as outpatients and were available for two follow-up examinations, after 2 weeks and after 12 weeks. Subjective evaluation was used to assess satisfaction of the patients. The evaluation was undertaken by questioning the patients, using the following criteria.
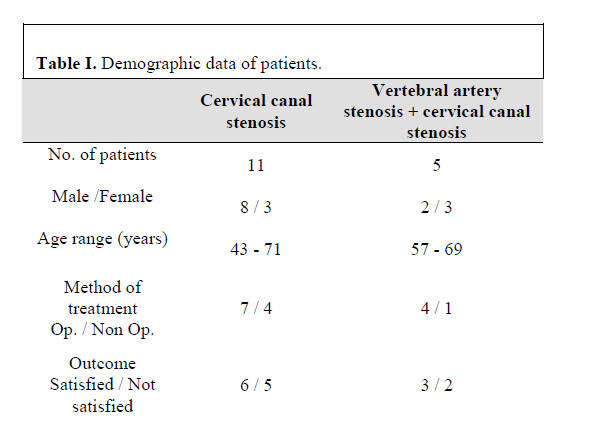
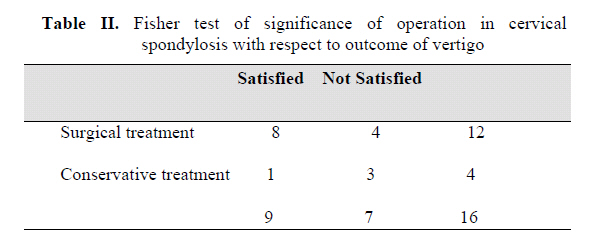
In the female group mean age was 60.3 years (49 - 65 years) and in the male group mean age was 65.2 years (57 - 72 years). Vertigo was the most common symptom (sixteen patients; 100%). Tinnitus was present in four patients (25%), myelopathy in ten patients (62.5%), mild hearing loss in one patient (6.2%) and radiculopathy in one patient (6.2% ). From sixteen patients with cervical spondylosis, twelve cases had cervical canal stenosis. Only two patients of this group had symptoms of vertebral artery stenosis. In four remaining patients, two cases had vertebral artery stenosis after rotation of the cervical spine. Operation was performed in twelve patients (75%) and conservative treatment with traction and collar in four patients (25%). (Table I) The results of surgical treatment were satisfactory in eight patients and unsatisfactory in the four remaining cases. Conservative treatment improved symptoms in one patient and did not improve three patients. Statistical analysis was performed using Fisher test which proved significance, in comparison between results of surgical versus conservative treatment of vertigo (Table II). DISCUSSION In cervical spondylosis the primary event is a progressive decrease in hydration of the nucleus polposus resulting in loss of disc height, disc fibrosis and weakening. The extra mobility between adjacent vertebral areas probably results in osteophyte formation. Although spur formation may attempt to stabilize the joints, their growth can result in narrowing of the spinal canal and compression to adjacent neurovascular structures. The responsible pathologies for this disorder are spondylotic spurs, cervical canal stenosis, and vertebral artery compression.7 There is potential association between cervical spondylosis and vertigo due to vertebrobasilar insufficiency.8,9 Vascular compromise by compression of the anterior spinal and radicular arteries and veins may be responsible for ischemia of the cord and not improve without surgery.10 Surgical treatment of cervical radiculopathy was associated with a better control of pain at 3 months, but conservative management had similar results during one year11, but these findings do not apply for vertebrobasilar insufficiency secondary to spondylosis. The most common pathology in our patients was canal stenosis and spondylotic spurs with vascular impingement. Transverse foraminotomy with drilling of spondylotic spurs is the most beneficial choice of treatment for rotational vertebral artery occlusion (RVAO) caused by spondylotic spur formation because it does not alter mobility of the cervical vertebra.12,13 In severe cervical stenosis with vertigo and other clinical findings, the best operation is laminectomy and foraminotomy and resection of spondylotic spurs and decompression of the cord and vascular elements.14,15,16,17 In our study, good results were achieved postoperatively after surgical intervention in three patients with RVAO. Conservative treatment had fair results in one patient with RVAO. CONCLUSIONVertigo may be present in cervical spondylotic patients, especially old cases with spondylosis. In most cases we recommend operation for decompressing the cord and arteries in the cervical spine. REFERENCES
Copyright 2006 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr06016f1.jpg] [mr06016t1.jpg] [mr06016t2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}