 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
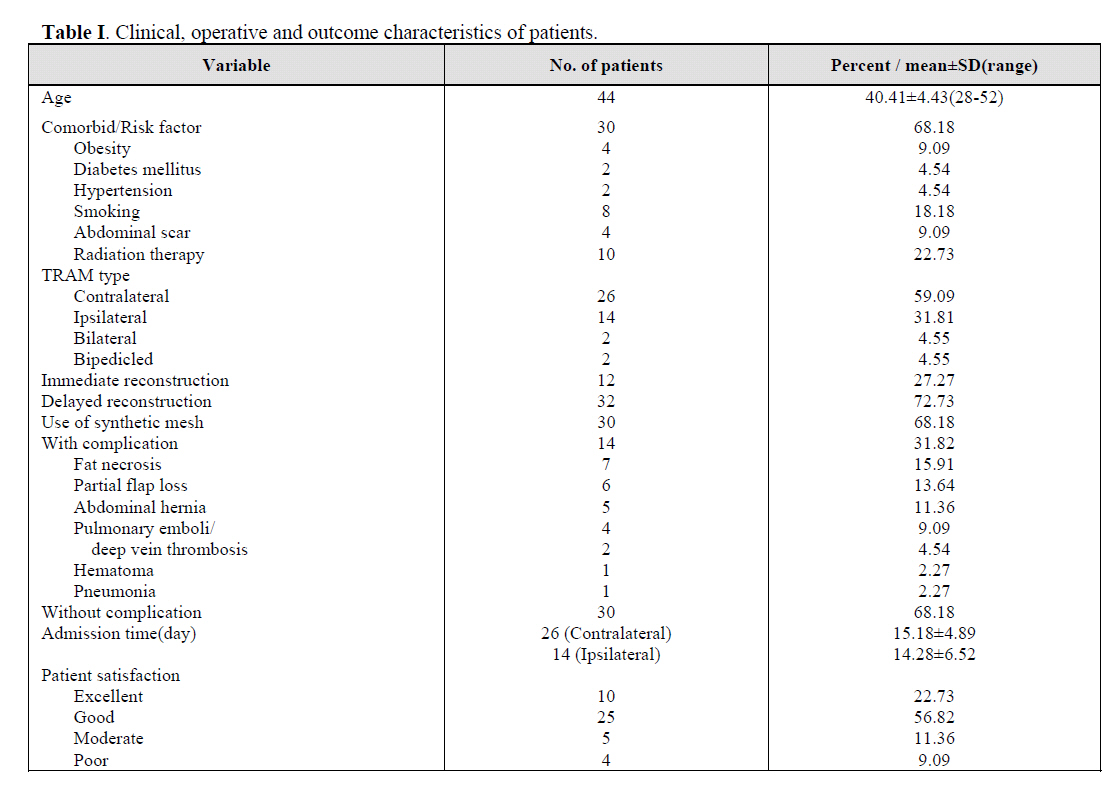
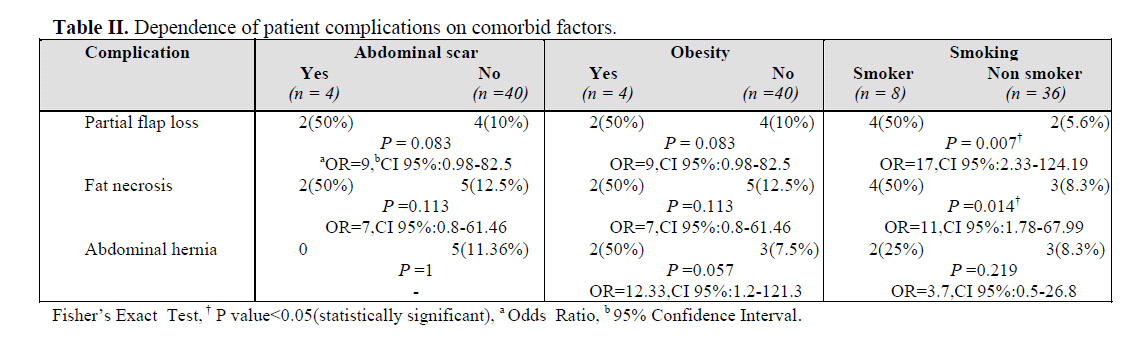
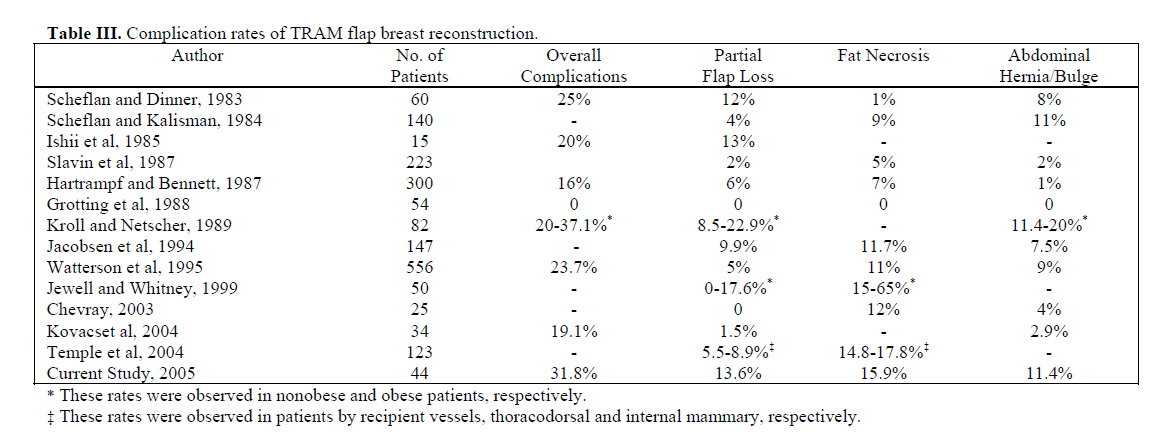
Medical Journal of the Islamic Republic of Iran , Vol. 20, No. 2, July, 2006, pp. 74-81 BREAST RECONSTRUCTION USING TRAM FLAP: PROSPECTIVE OUTCOME AND COMPLICATIONS MEHDI FATHI, MD*, EBRAHIM HATAMIPOUR, MD, HAMID R. FATHI, MD, AND HOMAYOON ZEHTAB, MD. From the Department of Plastic Surgery, Tehran University of Medical Sciences, Imam Khomeini Hospital, Keshavarz Ave., Tehran, Iran. Code Number: mr06018 ABSTRACTBackground: The transverse rectus abdominis musculocutaneous (TRAM) flap remains the gold standard for postmastectomy reconstruction either immediate or delayed. However, transfer of TRAM flap can be associated with donor site morbidities and complications in flap. A successful reconstruction consists of careful patient selection, surgical technique and meticulous preoperative planning. This study was designed to evaluate outcome and complications of breast reconstruction with TRAM flap in association with patient conditions and risk factors, prospectively. Keywords: Breast reconstruction, Transverse rectus abdominis myocutaneous (TRAM) flap, Complication. INTRODUCTION In the management of breast cancer - one of the most common malignancies in females - psychological aspects of mastectomy can be disappointing, as well as the fear of a potentially life - threatening disease. Since the novel development in breast reconstruction was introduced in early 1980s, a variety of pedicle or free flaps of the lower abdomen have been applied.1-4 However, the free transverse rectus abdominis musculocutaneous (TRAM) flap remains the gold standard, and others including deep inferior epigastric artery perforator (DIEP) and superficial inferior epigastric artery (SIEA) are indicated if their vessels could supply appropriate anatomic criteria.5 The TRAM flap rarely needs a silicone breast implant, is thought to result in a more natural - looking reconstruction and also removes excess tissue and fat from the abdomen.6 Direct microvascular anastomosis of free flaps have been performed for nearly 20 years, and offered better and more predictable perfusion. In addition, native shape of breast and shorter scar has been attained using a combination of free tissue transfer with further refinements in skin - sparing mastectomy.7 In designing the free TRAM flap, it is essential to determine in advance which part will best simulate the opposite breast. An ipsilateral flap can create a breast mound with more inferior fullness and ptosis, while a contralateral flap can be shaped into a full, conical breast yielding more projection.5 In the conventional TRAM flap, blood supply is derived from the superior epigastric system. The improved blood supply of the free TRAM flap is based on the more dominant inferior epigastric vascular pedicle, which allows for the transfer of larger volumes of tissue with minimal risk of fat necrosis.8 Harvesting of the pedicled TRAM flap can be associated with considerable donor site morbidity, as well. Postoperative abdominal hernia and bulges have been reported, and the strength of the abdominal wall and back muscles is decreased.9, 10 However, the free flap techniques have been the topic of much discussion and controversy that has been primarily based on the complexity of these operations, risk of total flap failure, financial considerations, and patient's satisfaction and quality of life. A successful reconstruction starts with careful patient selection, surgical technique, meticulous preoperative planning and postoperative hemodynamic monitoring. Some comorbid factors can not be optimized, including the effects of prior mastectomy and axillary lymph node dissection, prior chest wall radiation therapy, serious medical comorbidities, and advanced patient age.11, 12 Therefore, assessment of the risk of postoperative complications is a critical step, and the patients should be educated about their risk factors, such as smoking, hypertension, and diabetes. This study was designed to evaluate outcome and complications of breast reconstruction with TRAM flap in association with patient's conditions and risk factors, prospectively. PATIENTS AND METHODS Patient selectionBreast reconstruction was performed in 44 women consecutively, using autologous tissue from the lower abdomen during a 3-year period from 1999-2002. Database of all the patients was collected during this time, prospectively. Modified radical mastectomy accompanying immediate reconstructions with TRAM flap was indicated for 12 patients in whom stage I cancer had been documented in pathological biopsy. The TRAM flap was used for delayed reconstruction for other patients with previous mastectomy. Different TRAM flaps were applied in patients, contralateral pedicled flap, using contralateral transverse rectus abdominis muscle via superior epigastric artery, ipsilateral pedicle flap via ipsilateral superior epigastric artery and free TRAM flap via deep inferior epigastric artery. An assessment of soft tissue volume requirement of the breast was compared with the available tissue in the lower abdomen area. Surgical techniquePatients being in seated position, the limits of TRAM flaps were made preoperatively; the upper limit was labeled above the umbilicus and the inferior limit was similar to abdominal lipectomy. In patients with immediate reconstruction, the breast was resected by modified radial mastectomy, then superior incision of musculocutaneous flap was made in supine position, and superior abdominal flap was removed. The operating table was flexed up to 60º and abdominal flap was stretched down to determine site of inferior incision. After that the operating table was returned to primary position, an inferior incision was made, and the contralateral flap was dissected medially for flap elevation. In this phase, we attempted carefully to conserve perforator vessels. The flap was dissected ipsilateral to the artery pedicle, and raised up to the anterior half of the rectus sheath. It was cut nearly between the pubis and the umbilicus. Deep inferior epigastric vessels were visualized and ligated. We conserved 30 percent of the rectus muscle, fascia and some medial parts. The area around the umbilicus was incised, and the flap was elevated over the superior epigastric artery. Cutaneous flap of chest wall was dissected and a medial wide tunnel was made to place the flap in an appropriate site. In delayed reconstruction, end - to - end anastomosis of superior or deep inferior epigastric vessels to internal mammary vessels were performed for most flaps. The thoracodorsal vessels were used for all immediate reconstructions following modified radical mastectomy. The abdominal defect was repaired using primary closure in medial and lateral of rectus muscle residue. A Prolene synthetic mesh (20×30 cm) was used in some patients, being sutured and fixed in the inferior part of the abdomen. All the TRAM flap transfers were performed by the same team of plastic surgeons. Postoperative care and follow-upPostoperative monitoring consisted of direct evaluation of the flap every 15 minutes while in the recovery room, every hour for the first 24 hours, and every 2 hours for the next 48 hours. Surface temperature, flap color and capillary refill were checked. All the patients were visited in the plastic surgery clinic and cancer institute of a tertiary hospital, every week for the first 3 months and every month during 6 months followup. The satisfaction rate for the patient was assessed by face to face questioning. Data AnalysisDescriptive statistics of demographic, clinical, reconstructive, outcome and complications were summarized as a mean ± SD or as percentage of patients having the characteristics. Statistical analysis was performed using Chi2 and student t tests for categorical and continuous data, respectively. Univariate analysis was performed on comorbid factors (smoking status, age>60, obesity, diabetes mellitus, hypertension, abdominal scar and radiation therapy), techniques of TRAM flap (ipsilateral contralateral delayed versus immediate) and use of synthetic mesh for the dependent variables (fat necrosis, partial flap loss, abdominal hernia, admission days). Risk estimate was calculated for the associated variables to comorbid factors using Odds Ratio with 95% Confidence Interval (CI 95%). Level of p<0.05 was considered as statistically significant. Statistical analysis was performed using SPSS version 11.5 (Chicago, Inc). Written informed consent was obtained from all the patients in this study. The medical ethics committee of the hospital approved the protocol. This study was conducted according to the tenets of the Helsinki Declaration and good clinical practices. RESULTSA total of 44 consecutive women underwent breast reconstruction using TRAM flap over a 3-year period. The mean age of the patients was 40.41±4.43 years. Thirty (68.18%) patients had comorbidities, consisting of radiation therapy, obesity, hypertension, diabetes mellitus, smoking and abdominal scar. Contralateral and ipsilateral TRAM flaps were used in 26(59.09%) and 14(31.81%) reconstructions, respectively. Bilateral and/or bipedicled TRAM flap were used in the remaining four reconstructions. Twelve patients (27.27%) underwent immediate breast reconstruction, and 32(72.73%) patients underwent delayed reconstruction. The abdominal defect was repaired in layers with the use of synthetic mesh in 30 (68.18%) patients. The overall complication rate was 31.82%, consisting of fat necrosis (15.91%), partial flap loss (13.64%), etc. Satisfaction rates were excellent in 10 (22.72%), good in 25 (56.82%), moderate in five (11.36%), and poor in four (9.09%) patients. Clinical, operative and outcome characteristics of the patients are listed in Table I. Overall complications were 21 times more common in patients with comorbid factors compared with patients without morbidity (69.23% versus 3.23%, p<0.000, Odds Ratio = 67.50, 95%CI 6.67-683.06). There was no significant difference in the rate of complications (e.g., partial flap loss, fat necrosis, and abdominal hernia) between patients with and without history of radiation therapy (p>0.05). Also, the rate of complications had no association with type of TRAM flap (14.29% in contralateral versus 7.69% in ipsilateral) or interval from mastectomy up to reconstruction (37.5% in immediate versus 16.67% in delayed) (p>0.05). In patients in whom synthetic mesh was used, the rate of abdominal hernia was less compared with others (6.67% versus 21.14%, p = 0.15). The mean of postoperative inpatient hospital days were 15.18±4.89 and 14.28±6.52 in patients with contralateral and ipsilateral, respectively (p>0.05). From two breast reconstructions with bipedicled flap, one case developed fat necrosis. Patients with hypertension or diabetes mellitus had no complications. Relations between specific comorbid factors (abdominal scar, obesity and smoking), and the most common complications (partial flap loss, fat necrosis and abdominal hernia) are listed in Table II. DISCUSSIONOver the past decades, advancement of breast reconstruction with autologous tissue has changed surgical treatment trends in patients with breast cancer. In previous studies, psychosocial and physical benefits of breast reconstruction have been shown in patients undergoing mastectomy. In addition, it has been demonstrated that breast reconstruction is a safe, reliable operation that does not hide local recurrences or accelerate the rate or risk of breast malignancy spread.13-15 The National Health Service (NHS) Executive recommended that the possibility of reconstruction either immediate or delayed should be discussed with all women considering mastectomy.16 The most frequently used autologous tissue is the transverse rectus abdominis myocutaneous (TRAM) flap, whether pedicled or microsurgical breast reconstruction techniques are chosen.5 Also, the TRAM flap is well suited for immediate reconstruction because mastectomy and reconstruction can be performed simultaneously and symmetry and ptosis can be obtained in one operation.17 Direct microvascular anastomosis of free flaps have been performed for nearly 20 years, and offered better and more predictable perfusion. Careful patient selection, surgical technique and preoperative planning reduce postoperative complications. Some patient comorbidities have been considered to be a risk factor for postoperative complications, including prior mastectomy and axillary lymph node dissection, prior chest wall radiation therapy, serious medical conditions, advanced patient age and smoking.11, 12 In addition, harvesting of the pedicled TRAM flap can be associated with considerable donor site morbidity. Postoperative abdominal hernia and bulges have been reported, and the strength of the abdominal wall and back muscles is decreased. 9, 16 In our study of 44 consecutive patients following TRAM flap breast reconstruction, the outcome, complications and patient satisfaction were evaluated prospectively in a plastic surgery department of a tertiary hospital. All the patients were less than sixty years old. The rate of overall complications, fat necrosis, partial flap loss, abdominal hernia, pulmonary emboli/ deep vein thrombosis, hematoma and pneumonia was 31.82%. The most common complication was fat necrosis. Total flap loss, as the most serious complication of microsurgical breast reconstruction, occurred in no patients during their 6-month follow-up. Different techniques, contralateral, ipsilateral, and bilateral and bipedicled were used to prepare TRAM flaps for breast reconstruction as they were indicated. The differences of rate of complications and number of postoperative inpatient hospital days between types of TRAM flap techniques were not statistically significant, although the immediate reconstruction had better outcome and less complications compared with delayed reconstruction. Also, contralateral flaps resulted in fewer complications than ipsilateral flaps. The mentioned results were compatible with the experiences of other studies. Overall TRAM flap complications have been reported from 16% to 41%. 12, 1728 Total flap loss or necrosis has been observed in 0 to 9%.11,17,19,24,25 and 27 When it is possible, immediate reconstruction is more convenient for patients, and limits exposure to anesthesia risk. Also, aesthetic results tend to be better and the patient does not have to live with any deformity. Immediate breast reconstruction often permits shorter incisions with less skin removal. Also, the inframammary fold can be left intact in the immediate reconstruction. Many plastic surgeons agree that this procedure is technically easier than delayed reconstruction. However, the timing of reconstructive surgery may be influenced by hospital systems, patients' condition and need for radiotherapy. Optimal results are possible when both skin-sparing mastectomy and immediate breast reconstruction are present.4, 5, 15 and17 In delayed reconstruction, anastomosis failure of the flap is most likely related to its frequent association with previous axillary lymph node dissection and/or radiation therapy resulting in perivascular fibrosis, although the rate of flap failure had no significant differences between immediate and delayed approach.11 In one series, no significant difference in the incidence of early complications was found between patients who underwent delayed free TRAM flap reconstruction after the completion of radiation treatment and patients who had an immediate free TRAM flap prior to radiation. However, the incidence of late complications (fat necrosis, partial flap loss, flap contracture) was significantly higher in the immediate reconstruction group than in the delayed reconstruction group.29 Bipedicled TRAM flap is retained for patients with a limited amount of abdominal tissue, large breast and unwillingness to accept reduction of the contralateral breast and for those who have lower midline abdominal scarring. Incorporation of a second vascular pedicle into the flap may enhance the blood supply to the additional volume of tissue.15 In a retrospective study, medical records of breast reconstructions using unipedicled and/or bipedicled flap transfer in a conventional technique versus microsurgical technique have been reviewed. Patients who received a bipedicled TRAM flap using microsurgical technique appeared to have better flap perfusion and less abdominal hernia or bulging than did patients who underwent flap transfer using conventional technique. However these differences were not statistically significant.24 Actually, the increased dissection necessitated by such a bipedicled technique may increase donor-site morbidities. Compared unipedicled and bipedicled TRAM flap, subjective decrease in abdominal muscle strength was reported less in patients with one pedicle flaps.23, 30 In current study, two patients underwent bipedicled TRAM flap for unilateral breast reconstruction. One of the cases developed fat necrosis of the transferred flap. However, this obese patient had lower midline abdominal scarring because of resection of ovarian malignancy. It has been shown that TRAM flap transfer can create a weakness in the abdominal wall because of the harvest of rectus abdominis muscle and anterior fascia. Postoperative abdominal bulge and hernia can occur in up to 19% of cases. Some of these problems can be reduced by harvesting as little anterior rectus sheath and muscle above the arcuate line as possible. The muscle-sparing harvest of the rectus abdominis theoretically minimizes violation of the abdominal wall and the risk of donor site morbidity.9, 10, 31- 33 Other modifications in the technique of harvesting the lower abdominal flaps have been advocated, such as fascia-sparing, free TRAM, and the use of synthetic mesh to achieve a stable donor site. Whereas true hernia is less frequent today, bulging of the donor site, contralateral side or epigastric area is still a problem.10, 34 - 36 Predisposing factors which are mentioned for abdominal wall complications include nonselective vascular pedicle harvest, failure to close the anterior rectus sheath directly, the elderly attenuated abdominal wall, obesity, chronic pulmonary disease, smoking, and hypertension.37 The progressive reduction of abdominal hernia following flap transfer has been ascribed to increased experience of the surgeon and the more frequent use of synthetic mesh. The use of prosthetic mesh as an overlay graft for reinforcement of the primary closure in 40% of bipedicled and bilateral cases has been advocated, while other authors described the routine use of synthetic mesh for abdominal wall closure.35,39 Applying a mesh across the midline, with no anchoring superiorly and inferiorly can not prevent abdominal and epigastric bulging in areas where the mesh was not applied. This complication results from an uneven abdominal barrier facing internal abdominal pressure. The extended mesh provides a secure and permanent additional reinforcement to the entire abdominal wall, so may prevent hernia as well as bulging. In a study of patients who underwent breast reconstruction with conventional TRAM flap, using marlex or prolene mesh resulted in no true hernias, infections or seroma, and only one case of lower abdominal bulging36. In the current study, the rate of abdominal hernia in patients in whom synthetic mesh was used to repair the abdominal defect, was less than it was in patients without use of mesh, although this difference was not significant. Another purpose of this study was to evaluate comorbid and possible risk factors of the patients and determine whether there was an association between complications and these factors. The impact of radiation on vessels and tissue has been well documented. Perivascular fibrosis, endothelial damage and microvascular occlusion can impair the quality of recipient vessels.40 The impaired endothelial-dependent vasodilation may be related to slow recovery from vasospasm that can lead to vessel thrombosis.11 However, association between history of chest-wall irradiation and complications of transferred TRAM flap is inconsistence in previous studies. In a study of vascular anatomy of the TRAM flap and risk factors associated with complications, 556 women were evaluated. Fat necrosis of the flap associated with a history of chest-wall radiation therapy.22 While in the other two studies, no patterns of increased complications were noted in patients who had received preoperative irradiation.25, 41 We observed no significant difference in the rate of complications between patients with and without history of radiation therapy, although patients who had undergone chest wall irradiation have developed more fat necrosis and abdominal hernias. The internal mammary and thoracodorsal vessels are most commonly used for recipient vessels in microsurgical breast reconstruction. A diameter of 0.99 to 2.55 and 0.64 to 4.45 mm for internal mammary artery and vein, respectively, has been demonstrated. The diameter of the thoracodorsal vessels ranges from 1.5 to 3 mm for the artery and 2.5 to 4.5 for the vein.42 In previous studies, both vessels were suitable for microvascular anastomosis and no association was detected between choices of recipient vessels flap complications.11, 25, 43 and 44 Our results were compatible with these studies. However, thoracodorsal and internal mammary vessels were applied for immediate and delayed breast reconstruction. Two patients with hypertension and another two patients with diabetes mellitus developed no complications. The patients with history of hypertension were normotensive during the perioperative period. Also, diabetic women have an appropriate glycemic control and moderate insulin requirement, preoperatively. It has been documented that diabetes mellitus is associated with microangiopathic changes in both experimental and clinical studies. When glucose levels are well controlled, patency of the anastomosis is less affected and diabetic patients are not at increased risk for flap failure or complications.11, 45- 47 Obesity >125% ideal body weight, as defined a weight of 45.4 kg for 152.4 cm and an additional 0.94 kg for each cm above 152.4 cm, significantly increased the risk of partial flap loss and abdominal hernia, and marginally yielded more fat necrosis of the transferred TRAM flap. Previous studies have demonstrated an increased incidence of flap necrosis and abdominal wall hernia in obese patients comparing with nonobese candidates for TRAM flap transfer. Especially, morbidly obese patients who undergo breast reconstruction are at risk of flap necrosis as well as lower abdominal discomfort and hernia.26, 48 ,49 Despite obesity having been associated with any complication of breast reconstruction using TRAM flap22, 50, it has been reported that no significant difference was observed in the incidence of complications when assessed for overweight.25 Recently, a midabdominal TRAM flap was proposed as an option of breast reconstruction in the morbidly obese patients.26 In this study, it was mentioned that supply of musculocutaneous perforating and midline vascular vessels is more limited and there is loss of rectus musculofacial by dividing the rectus abdominis muscle at a level below the arcuate line, so patients who undergo transfer of conventional TRAM flap are predisposed to flap necrosis and abdominal hernia. Total complications of midabdominal TRAM flap were comparable to previous studies. In the current study, abdominal scarring due to previous midline incision or multiple incisions increased the incidence of partial flap loss. Previous abdominal surgery has been considered as a risk factor for complications following breast reconstruction with pedicled TRAM flap.18, 21 As it was mentioned bipedicle TRAM flap has been recommended for those with lower midline scarring.15 The overall complication rate for TRAM flap transfer has been associated with significant abdominal scarring.22 In contrast, it has been shown that complication rates of breast reconstruction with TRAM flap had no significant difference between patients with preoperative risk factors, such as scars of previous operations, overweight and smoking, and patients without these comorbidities.25 Smoking is generally considered as a risk factor for postoperative wound healing. The vascular manifestations associated with smoking include development of atherosclerosis, vasoconstriction, and platelet adhesion.51, 12, 11 However, tobacco use had different effect on surgical procedures such as abdominoplasty and autologous breast reconstruction. Some studies have shown that tobacco use was a significant risk for flap and donor site complications.11, 22, 52, and 49 While others have shown no associations between smoking and postoperative complications of flap transfer,41, 53, 54 we found that smoking increased the risk of fat necrosis and partial flap loss significantly. It is not clear what period of cessation time is needed to decrease the risk of surgical complications. It appears that ex-smokers had more complications comparing with smokers and/or women who had stopped smoking from 5 years to 3 months before reconstruction. However, the analysis of subgroups of smokers was not performed. This inconsistency in the literature may be due to different study design, and effects of confounders. The complication rate of breast reconstruction compared with previous studies have summarized in Table III. Patients who underwent breast reconstruction with TRAM flap felt a considerable improvement in the quality of life and self-consciousness. The rate of our patients' satisfaction was compatible with previous studies.19, 41 Up to 91% of our patients had acceptable flap success. Although breast reconstruction using autologous tissue may result in a more natural feel, natural looking reconstruction, patient satisfaction is based on multiple factors.19, 55, 56 One of the limitations of our study was the shortness of the follow-up period, therefore the recurrence rate of breast cancer was not studied. Also, multivariate analysis was not performed to determine the risk of any comorbidities for complications, because the rate of these factors was not enough to have a reasonable logistic regression. We obtained only the interventional group using flap transfer and patients with only mastectomy was not evaluated, especially considering measure of psychological well-being. CONCLUSIONThe outcome of breast reconstruction using TRAM flap is similar by surgical technique and time of reconstruction. The most common flap complications were fat necrosis and partial flap loss that were associated with smoking. Acceptable satisfaction is obtained by TRAM flap as the choice of flaps for breast reconstruction. REFERENCES
Copyright 2006 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr06018f3.jpg] [mr06018t3.jpg] [mr06018t2.jpg] [mr06018t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}