 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Medical Journal of the Islamic Republic of Iran , Vol. 20, No. 2, July, 2006, pp. 82-85 JEJUNAL EVERSION MUCOSECTOMY AND INVAGINATION: AN INNOVATIVE TECHNIQUE FOR THE END TO END PANCREATICOJEJUNOSTOMY ALIREZA KALANTAR MOTAMEDI, MD. From the Department of General and Vascular Surgery, Hazrat Rasool Medical Complex, Iran University of Medical Sciences, Tehran, IRAN. Code Number: mr06019 ABSTRACT
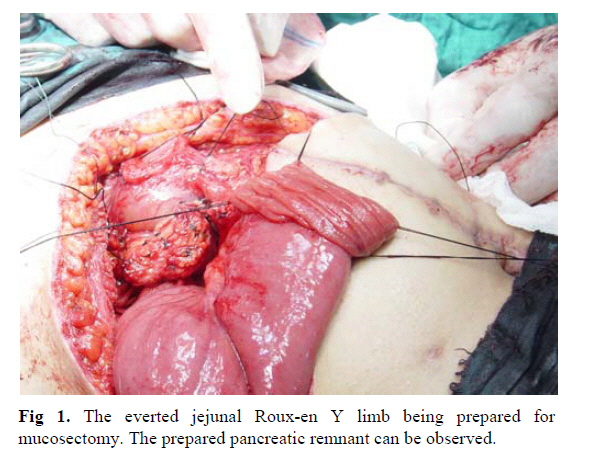
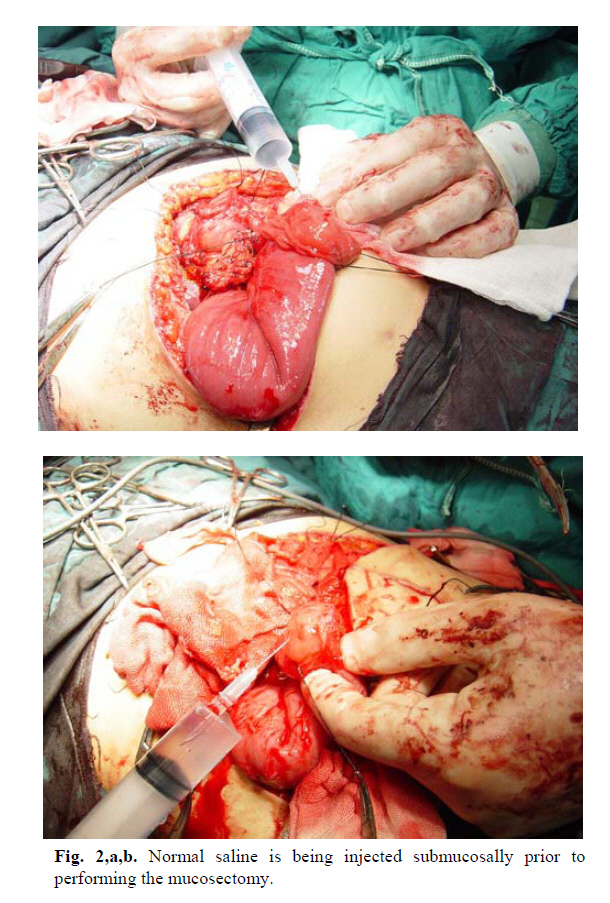
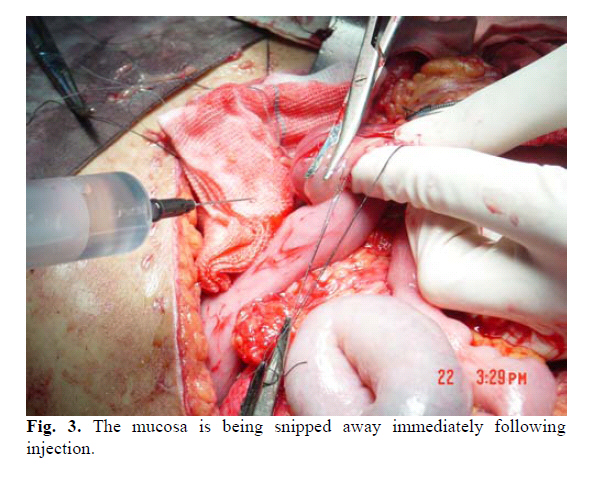
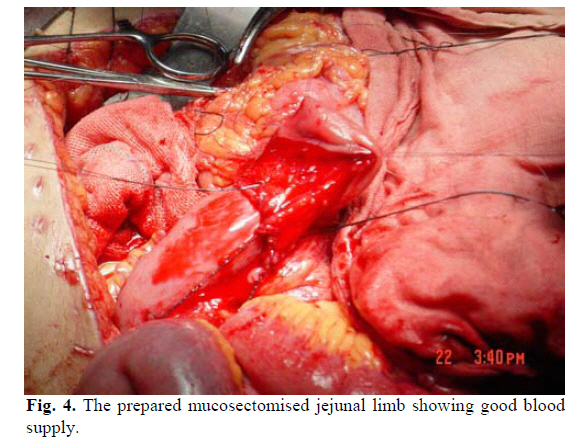
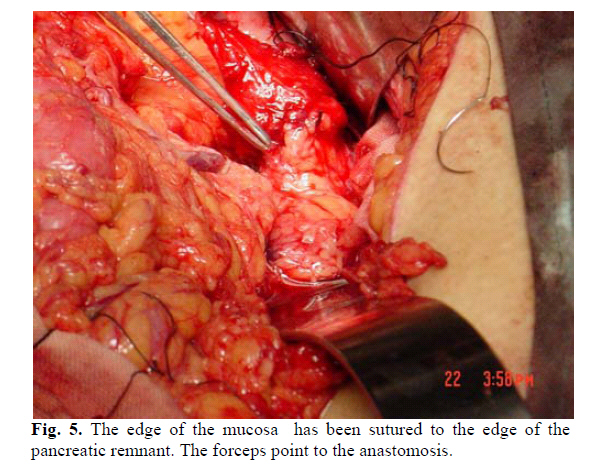
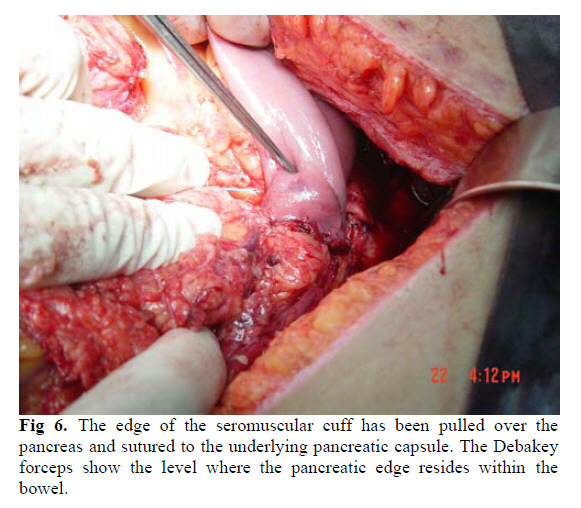
Background: The pancreatojejunostomy has notoriously been known to carry a high rate of operative complications, morbidity and mortality, mainly due to anastomotic leak and ensuing septic complications. INTRODUCTION The pancreaticojejunostomy is probably one of the most problematic anastomoses known to surgeons worldwide, and anastomotic leak is much more commonly observed in this procedure compared to other GI anastomoses. The impact and deleterious effect and subsequent morbidity of postoperative anastomotic leak is especially significant in elderly patients with periampullary carcinoma. Such patient groups usually tolerate major operations well, but do poorly when afflicted with complications. At the least, pancreatic fistulas are associated with a significant prolongation of postoperative hospital stay. Various techniques have been proposed by authorities for performing the pancreaticojejunostomy, consisting of end-to-side or end-to-end methods, duct-to-mucosa sutures and invagination. Others have recommended performing a pancreaticogastrostomy. Regardless of the technique or method used, the pancreatic leakage rate has always been reported to be around 10% in specialized centers, ranging from 5.8% to over 20%1,9,10,11 and much higher in departments with less experience and a smaller number of patients undergoing pancreatic surgery, i.e., the Whipple procedure. It is common belief that this 10% leak rate is inevitable and must be accepted on behalf of the surgeon and patient as an unpreventable complication just waiting to happen. A new anastomotic technique pioneered by the author and used for the past 4 years has proven to be trustworthy in leak prevention to date, as not a single case in the author's group undergoing a pancreaticojejunostomy following pancreaticoduodenectomy developed a pancreatic fistula postoperatively. PATIENTS AND METHODSFrom a total of 18 patients within a 4 year time period, 14 cases underwent pyloric-saving pancreatoduodenectomy for periampullary carcinoma, one for papillary epithelial neoplasm, two patients with ampullary avulsion/severe pancreatoduodenal trauma, and one patient with a proximal pancreatic fistula who underwent distal pancreatectomy and a Roux-en-Y pancreatojejunostomy to the remnant proximal pancreatic head which had a large pancreatic duct in order to hasten fistula closure by facilitating pancreatic drainage. OPERATIVE TECHNIQUEFollowing a formal pancreatico-duodenectomy with or without saving the pylorus, a Roux-en-Y limb of jejunum is prepared and brought adjacent to the pancreatic remnant. Using babcock forceps, the jaws of the instrument are inserted 3-4 cm inside the jejunal limb and the full thickness of the bowel is grasped and everted inside-out. Four mucosal stay sutures of 3/0 vicryl are then inserted at the four quadrants of the circumference of the bowel, 2 cm from the bowel end. These four sutures define the limit of the mucosectomy. Four 3/0 vicryl stay sutures are then inserted at the bowel edge of the jejunal limb. Afterwards normal saline is injected submucosally using an 18 gauge needle and 20 mL syringe in the predefined 2 cm area to expand the submucosal space and prevent injury to the submucosal vessels and bowel wall vasculature when performing the mucosectomy. After injection, the mucosa is snipped away using Metzenbaum scissors, taking care not to cut deep and button-hole the everted bowel wall. Normal saline injections are repeated as needed during the procedure, until a completely mucosectomised cuff of seromuscular bowel tissue remains extending for 2 cm from the edge of the jejunum. Next the surgeon must prepare the pancreatic remnant such that 2 cm of it is free from peripancreatic fat and adjacent tissues. At this point the mucosal edge of the everted jejunal limb is sutured with the previously placed vicryl stay sutures to the edge of the pancreatic remnant, with added vicryl sutures as necessary in between. Then the 2 centimeters of everted seromuscular cuff is pulled over the pancreas, much in the way that one pulls a stocking up one's leg, to cover 2 cm of pancreatic capsule and sutured to the pancreatic capsule with the previouslyplaced bowel edge sutures of 3/0 vicryl. As an added but probably unnecessary safety measure, a tongue of omentum is wrapped around the anastomosis in order to separate the superior mesenteric vein from the pancreas. The hepaticojejunostomy is then done in an end to side fashion using conventional techniques, as is the duodenojejunostomy in cases where a radical pancreaticoduodenectomy has been performed. The author routinely places closed suction Hemovactype drains near the pancreatic and hepatic duct anastomoses. These are usually removed in a few days. POTENTIAL TECHNICAL BENEFITS of this innovative technique include:
From a total of 18 patients, 16 patients had an uneventful postoperative course with no anastomotic leak, and only one episode of delayed gastric emptying occurred which was managed conservatively. We had one mortality on PO day 3 due to an extensive myocardial infarction. Hemovac drains were removed on PO day 3 or 4, at a time which drainage of peritoneal fluid had become negligible, and all patients were discharged on PO day 6, except for the patient with delayed gastric emptying who was discharged on PO day 12. DISCUSSION Reported risk factors for anastomotic leak include surgeon inexperience, soft pancreatic texture, and, if performed, ligation of the pancreatic duct4. Patients with small, unobstructed pancreatic ducts or soft, friable pancreata are at particularly high risk5. The pancreaticogastrostomy has also not been shown to have a lower risk of anastomotic leak compared to the conventional pancreaticojejunostomy6. Octreotide has also proven to be ineffective in this regard 7. Out of frustration, some have even attempted to accept a controlled pancreaticocutaneous fistula after pancreatic resection, the outcome of which was shown to be better than that which a patient were to suffer should he or she develop a leak following pancreatojejunostomy8. CONCLUSIONAccording to the above, pancreatic anastomotic leak appears to be a preventable complication. This technique appears promising and is gaining popularity in our institution, and is therefore recommended as a choice method for any operation requiring a pancreaticojejunal anastomosis. We believe the occurrence of no case of pancreatic fistula in any of the 18 cases operated is reason enough to consider this method as a first line technique in all such operations. Obviously, a larger number of cases and multicenter trials in the future will determine whether this technique can surely and predictably prevent this difficult complication from occurring in patients undergoing pancreaticoduodenectomy for benign or malignant disease. REFERENCES
Copyright 2006 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr06019f6.jpg] [mr06019f2.jpg] [mr06019f5.jpg] [mr06019f4.jpg] [mr06019f3.jpg] [mr06019f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}